
You've done the research. You've picked your supplements carefully. But here's the part most people skip: checking whether those supplements actually play well together.
The truth is, taking the wrong combination of supplements — or mixing certain supplements with prescription medications — can quietly undermine everything you're trying to accomplish. In some cases, the stakes go well beyond reduced absorption. We're talking about interactions that can land you in the emergency room.
Consider this: St. John's wort, a popular natural antidepressant, is a potent inducer of CYP3A4 enzymes and P-glycoprotein, which means it can drastically reduce the effectiveness of birth control pills, blood thinners, HIV medications, and immunosuppressants. Or take something as seemingly harmless as a calcium supplement — when taken alongside iron, it can slash iron absorption by 30–50%. And long-term zinc supplementation above 60 mg per day? That can deplete your copper stores enough to cause anemia and neurological damage.
These aren't fringe scenarios. They happen to real people who simply didn't know what not to combine.
This guide breaks down every major supplement interaction you need to know about — the mineral competitions, the enzyme hijackers, the medication conflicts — and gives you a clear, practical spacing schedule so you can take your supplements safely. If you're also wondering about optimal timing, check out our supplement timing and absorption guide.
For a deeper understanding of individual supplements discussed here, see our guides on zinc, iron, calcium and bone health, and magnesium.
What Are Supplement Interactions and Why Should You Care About Them?
Supplement interactions occur when two or more supplements — or a supplement and a medication — interfere with each other's absorption, metabolism, or biological activity. These interactions can reduce effectiveness, amplify side effects, or create entirely new health risks. With over 50% of American adults taking dietary supplements, and many combining multiple products with prescription drugs, understanding these interactions is a genuine safety issue.
There are three main categories of supplement interactions, and each works through different mechanisms.
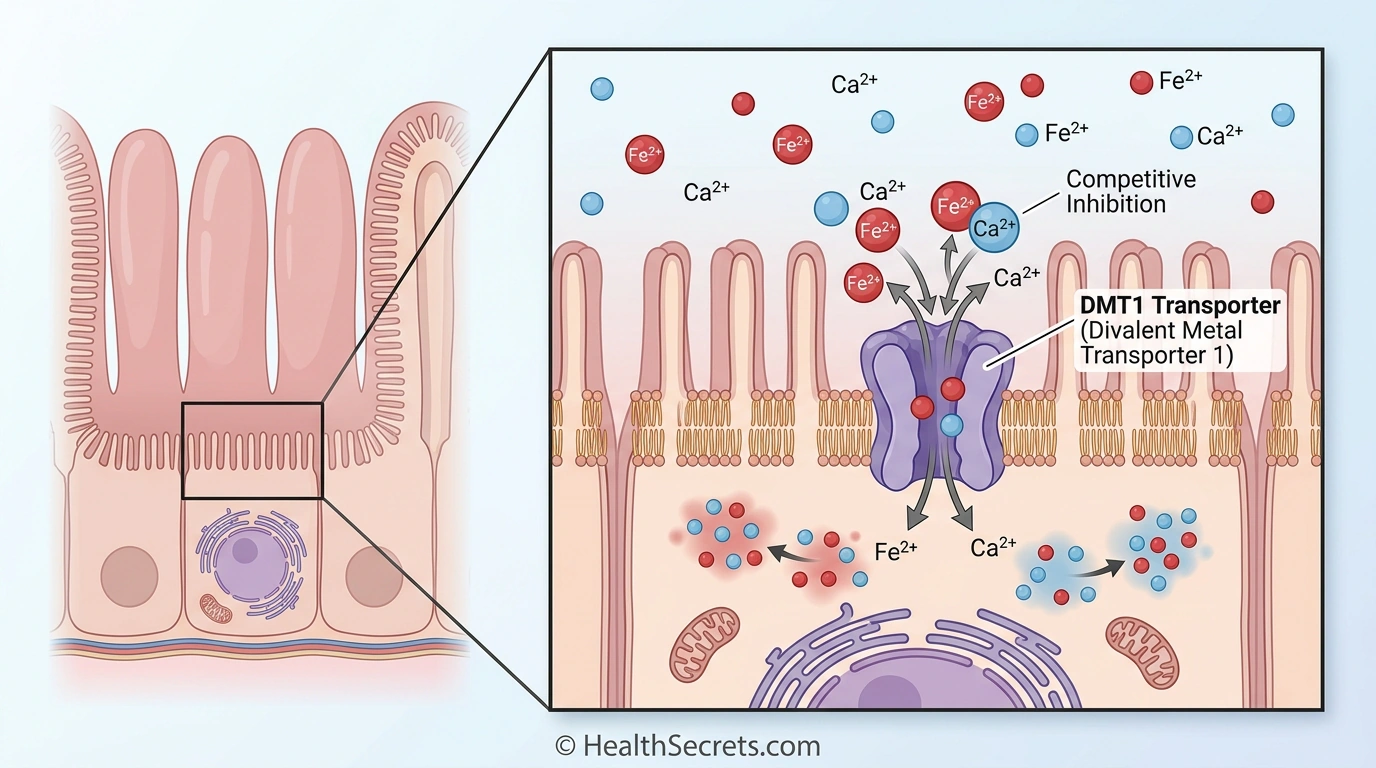
- Supplement-to-supplement interactions happen when nutrients compete for the same absorption pathways. Calcium and iron, for instance, both use the divalent metal transporter 1 (DMT1) in your intestinal lining. When they arrive at the same time, they're essentially fighting over the same doorway into your bloodstream.
- Drug-supplement interactions are often more dangerous. Some supplements alter how your liver processes medications — speeding up or slowing down drug metabolism through the cytochrome P450 enzyme system. Others physically bind to medications in your gut, preventing them from being absorbed at all.
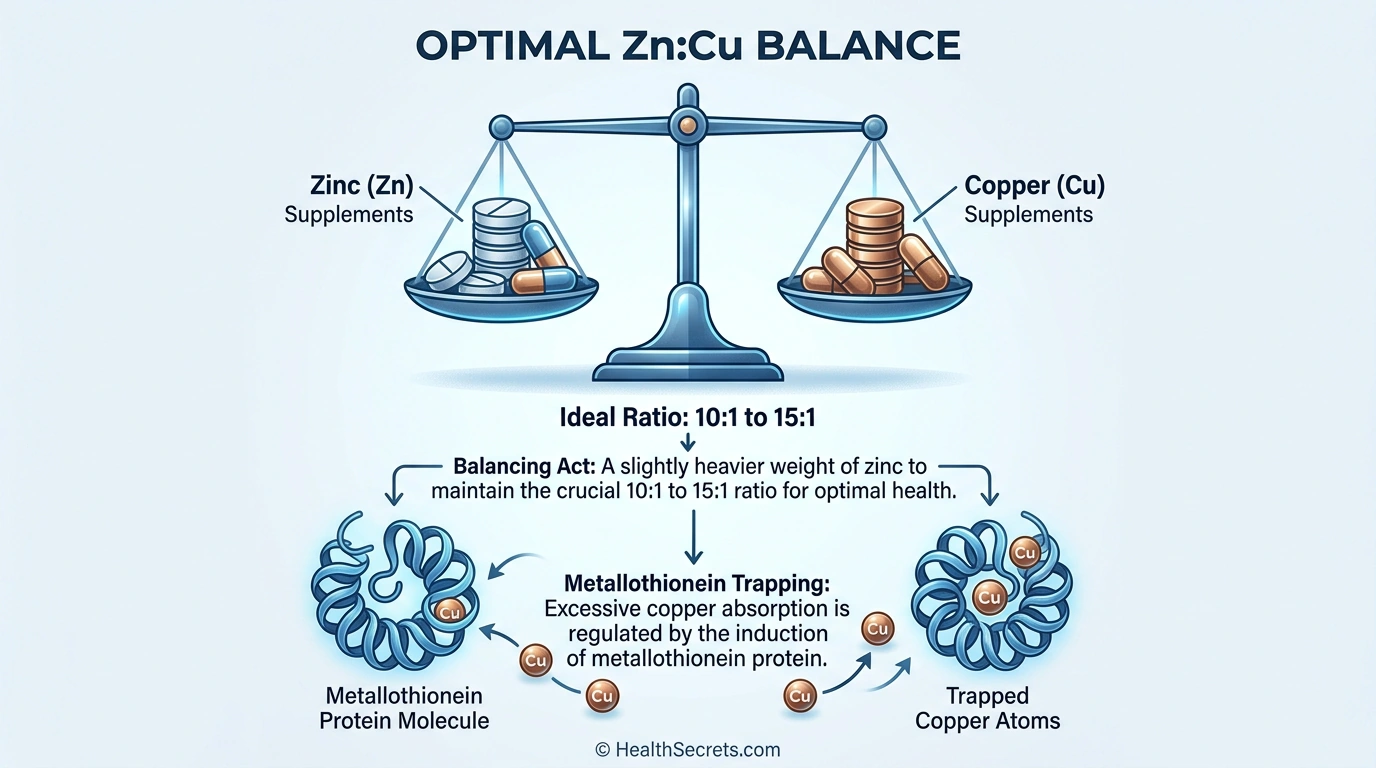
- Nutrient depletion interactions occur over weeks or months, where one supplement gradually depletes another. High-dose zinc, for example, induces a protein called metallothionein that traps copper in your intestinal cells, slowly creating a copper deficiency that can take months to become apparent.
The good news? Most interactions are manageable once you know about them. Proper spacing, dose adjustments, and a few simple rules can prevent the vast majority of problems.
How Do Supplement Interactions Actually Happen in Your Body?
Supplement interactions operate through four primary biological mechanisms: enzyme induction, competitive absorption, chelation, and protein-mediated sequestration. Understanding these mechanisms helps you predict which combinations are problematic and why spacing or dose adjustments work as solutions.
How Does Enzyme Induction Cause Drug-Supplement Interactions?
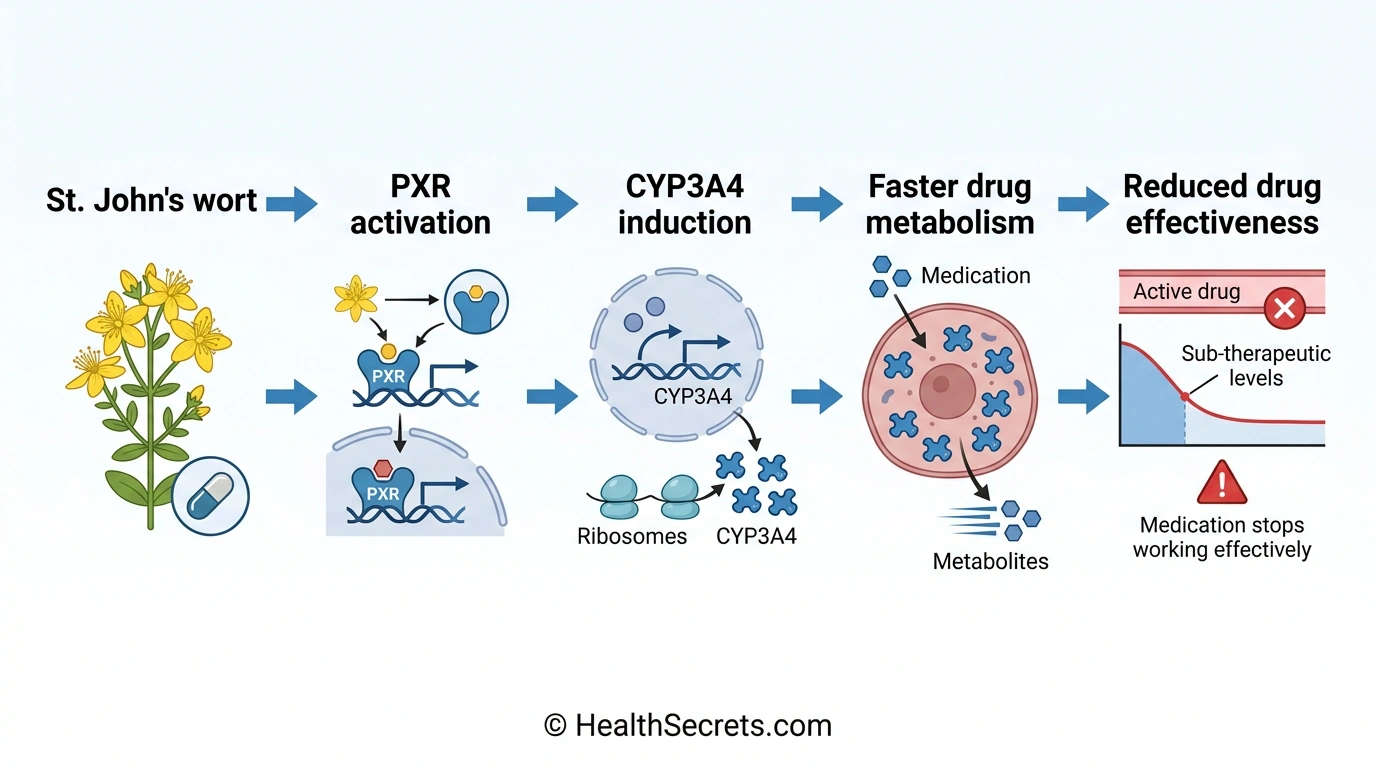
Enzyme induction is the most dangerous interaction mechanism because it can render life-saving medications ineffective. Certain supplements activate nuclear receptors — particularly the pregnane X receptor (PXR) — which ramp up production of drug-metabolizing enzymes in your liver.
St. John's wort is the prime example. Its active compound hyperforin is a potent PXR activator, which upregulates cytochrome P450 3A4 (CYP3A4) — the enzyme responsible for metabolizing roughly 50% of all prescription drugs. When CYP3A4 activity increases, medications are broken down faster than intended, reducing their blood levels and therapeutic effectiveness. St. John's wort also induces P-glycoprotein, a transporter protein that pumps drugs back out of cells before they can take effect.
How Do Minerals Compete for Absorption in Your Gut?
Many essential minerals are divalent cations — they carry a +2 electrical charge — which means they share the same intestinal transport proteins. The divalent metal transporter 1 (DMT1) in your duodenum doesn't strongly discriminate between calcium, iron, zinc, copper, and magnesium. When multiple divalent minerals arrive simultaneously, they compete for transport across the intestinal wall.
Calcium and iron compete intensely because both rely heavily on DMT1. Research shows calcium can reduce iron absorption by 30–50% in single-meal studies, though the body may develop compensatory mechanisms during long-term supplementation. Iron and zinc also compete — each reduces the absorption of the other when taken together.
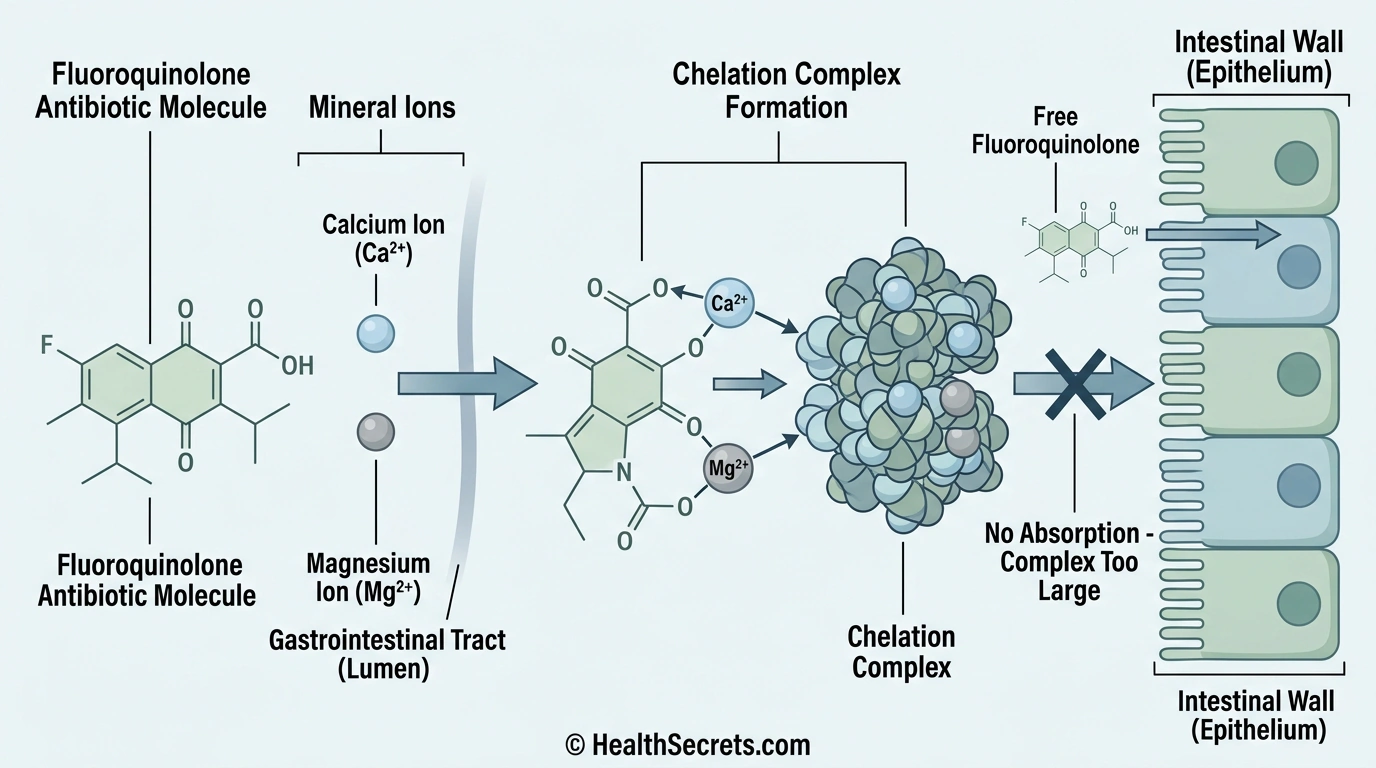
What Is Chelation and How Does It Block Medication Absorption?
Chelation occurs when mineral supplements form insoluble chemical complexes with medications in your gastrointestinal tract. The resulting complexes are too large to cross the intestinal wall, so both the mineral and the medication pass through unabsorbed.
This is particularly problematic with antibiotics. Fluoroquinolones (ciprofloxacin, levofloxacin) and tetracyclines (doxycycline, minocycline) have molecular structures that readily bind to calcium, magnesium, iron, and zinc. Calcium carbonate alone can reduce ciprofloxacin bioavailability by 40%. The same chelation mechanism explains why minerals interfere with thyroid medication — levothyroxine binds to calcium, iron, and magnesium in the gut, reducing thyroid hormone absorption.
How Does Metallothionein Cause Zinc-Copper Depletion?
Metallothionein is a small, cysteine-rich protein that your intestinal cells produce in response to zinc exposure. When zinc intake is high, metallothionein production increases dramatically. The problem? Metallothionein has an even stronger affinity for copper than for zinc. It traps copper inside intestinal cells, which are eventually shed and excreted — taking the bound copper with them. Over weeks to months of high-dose zinc supplementation, this process slowly depletes your body's copper stores.
What Are the Most Critical Supplement-to-Supplement Interactions You Need to Know?
The most important supplement-to-supplement interactions involve mineral competition for absorption pathways, nutrient depletion over time, and additive effects that increase bleeding risk. Knowing these specific pairs — and how to manage them — is the foundation of a safe supplement regimen. Most can be resolved simply by adjusting timing.
Does Calcium Really Block Iron Absorption?
Yes — calcium can inhibit iron absorption by 30–50% when the two are taken together in a single meal. The effect occurs because both minerals compete for the DMT1 transporter in the duodenum. However, research suggests this inhibition may be short-lived, with possible compensatory mechanisms involving ferroportin and hephaestin that kick in during long-term supplementation.
The clinical significance depends on your iron status. For people with iron deficiency anemia, pregnant women, or vegetarians with lower iron stores, this interaction genuinely matters. The solution is straightforward: take iron on an empty stomach (30 minutes before meals) with vitamin C to enhance absorption, and take calcium with a different meal — ideally lunch, dinner, or before bed. Calcium-rich foods like milk, cheese, and yogurt also reduce iron absorption, so avoid consuming them alongside your iron supplement.
How Does Long-Term Zinc Supplementation Cause Copper Deficiency?
High-dose zinc supplementation (above 40–50 mg daily) over weeks to months induces metallothionein in intestinal cells, which preferentially binds and traps copper. Case reports document patients developing copper deficiency anemia and neutropenia (dangerously low white blood cells) during long-term zinc therapy. The major consequence of chronic excessive zinc intake — total intakes above 60 mg per day — is copper deficiency, which can cause anemia, immune suppression, neurological problems, and bone abnormalities.
The fix: limit zinc supplementation to 15–30 mg daily unless medically supervised. If you need higher doses, supplement with 1–2 mg copper daily (roughly 1 mg copper per 8–15 mg zinc) to maintain a healthy zinc-to-copper ratio of approximately 10:1 to 15:1. Good food sources of copper include shellfish, nuts, seeds, organ meats, and dark chocolate.
Can You Safely Take Fat-Soluble Vitamins Together?
Generally, yes. Vitamins A, D, E, and K are all absorbed with dietary fat, and taking them together with a meal containing healthy fats actually enhances absorption across the board. There's one important exception: very high-dose vitamin E (above 1,000 IU) may interfere with vitamin K-dependent clotting factors, potentially increasing bleeding risk — especially concerning if you're on blood thinners.
At standard supplemental doses, there's no problem combining fat-soluble vitamins. Just make sure you take them with your fattiest meal of the day.
Does High-Dose Vitamin C Destroy Vitamin B12?
This is a theoretical concern that hasn't been convincingly demonstrated in clinical settings. Early studies suggested that very high-dose vitamin C (above 1,000 mg) might degrade B12 in the stomach. More recent research questions whether this occurs at physiologically relevant levels. Still, if you're taking both high-dose vitamin C and B12, a simple precaution is to separate them by 2 hours — or use sublingual B12, which bypasses the stomach entirely.
When Do Fish Oil and Vitamin E Become a Bleeding Risk?
Fish oil (omega-3 fatty acids) has a mild antiplatelet effect, and high-dose vitamin E (above 400 IU) also has blood-thinning properties. Individually, these effects are modest.
Combined — especially in someone already taking anticoagulant medication — the additive effect can increase bleeding risk. At normal supplemental doses (1–2 g fish oil, 100–200 IU vitamin E), the combination is generally safe for most people. But avoid high-dose vitamin E if you're taking fish oil alongside blood thinners.
Ezy Dose Weekly AM/PM Pill Organizer
Editor's ChoiceEzy Dose · Managing daily supplement spacing to avoid interactions
Thorne Zinc Picolinate 30 mg
Best for Safe Zinc DosingThorne Zinc · Moderate-dose zinc supplementation that minimizes copper depletion risk
Doctor's Best High Absorption Magnesium Glycinate 200 mg
Best for Evening DosingDoctor's Best · Standalone magnesium taken at bedtime, separated from calcium and other minerals
NOW Foods Iron 36 mg Double Strength (Ferrochel)
Best Standalone IronNOW Foods · Iron supplementation that can be precisely timed away from calcium and other minerals
NOW Foods Selenium 200 mcg
Best ValueNOW Foods · Standalone selenium with no significant mineral interaction concerns
Read the detailed review cards below before opening any retailer link
Top Recommended Products
Ezy Dose
Ezy Dose Weekly AM/PM Pill Organizer
The single most effective tool for preventing supplement interactions is a compartmentalized pill organizer. Pre-sorting your supplements weekly eliminates daily guesswork about timing.
Pros
- + AM/PM compartments enforce spacing
- + removable daily pods for travel
- + easy-open lids
- + affordable
Cons
- - Only 2 compartments per day — may need additional organizer for midday doses
Why we included it: The single most effective tool for preventing supplement interactions is a compartmentalized pill organizer. Pre-sorting your supplements weekly eliminates daily guesswork about timing.
Retailer link opens on Amazon after the review details above

Thorne Zinc
Thorne Zinc Picolinate 30 mg
At 30 mg, this stays below the 40 mg threshold where copper depletion becomes a concern. Picolinate form is well-absorbed, and NSF certification ensures label accuracy.
Pros
- + 30 mg dose stays within safe range
- + NSF certified
- + highly bioavailable picolinate form
- + no unnecessary additives
Cons
- - Does not include copper — add separately if taking daily long-term
Why we included it: At 30 mg, this stays below the 40 mg threshold where copper depletion becomes a concern. Picolinate form is well-absorbed, and NSF certification ensures label accuracy.
Retailer link opens on Amazon after the review details above

Doctor's Best
Doctor's Best High Absorption Magnesium Glycinate 200 mg
Taking magnesium at bedtime naturally separates it from calcium and iron taken earlier in the day. Glycinate form maximizes absorption and supports sleep quality.
Pros
- + Glycinate form is gentle on stomach
- + ideal for bedtime dosing away from competing minerals
- + high absorption
- + large count
Cons
- - Requires 2 tablets per serving
Why we included it: Taking magnesium at bedtime naturally separates it from calcium and iron taken earlier in the day. Glycinate form maximizes absorption and supports sleep quality.
Retailer link opens on Amazon after the review details above
NOW Foods
NOW Foods Iron 36 mg Double Strength (Ferrochel)
Standalone iron capsules let you take iron on an empty stomach in the morning with vitamin C, well-separated from calcium, zinc, and other competing minerals.
Pros
- + Chelated form minimizes stomach upset
- + can take on empty stomach
- + vegan-friendly
- + affordable
Cons
- - 36 mg may be higher than needed for maintenance — consult your provider
Why we included it: Standalone iron capsules let you take iron on an empty stomach in the morning with vitamin C, well-separated from calcium, zinc, and other competing minerals.
Retailer link opens on Amazon after the review details above

NOW Foods
NOW Foods Selenium 200 mcg
Selenium has minimal interaction concerns with other common supplements, making it a flexible addition to any properly spaced regimen.
Pros
- + No major absorption conflicts with other minerals
- + 6-month supply
- + yeast-free
- + affordable
Cons
- - High dose — don't combine with selenium-containing multivitamins to avoid exceeding 400 mcg daily upper limit
Why we included it: Selenium has minimal interaction concerns with other common supplements, making it a flexible addition to any properly spaced regimen.
Retailer link opens on Amazon after the review details above
What Are the Most Dangerous Drug-Supplement Interactions?
The most dangerous drug-supplement interactions involve St. John's wort with nearly any prescription medication, vitamin K with warfarin, mineral supplements with antibiotics and thyroid drugs, and blood-thinning supplements with anticoagulant medications. Unlike supplement-to-supplement interactions, these can cause treatment failure, organ rejection, or life-threatening bleeding — making them genuine medical emergencies.

Why Is St. John's Wort the Most Dangerous Supplement for Drug Interactions?
St. John's wort (Hypericum perforatum) is used to treat mild to moderate depression, but it interacts with more medications than almost any other supplement. Its active compound hyperforin is a potent activator of PXR, inducing CYP3A4 and P-glycoprotein at levels that significantly alter drug metabolism.
Clinically significant interactions have been identified with a startling range of prescription medications:
- Antidepressants (SSRIs, SNRIs, MAOIs): Risk of serotonin syndrome — a potentially fatal condition. Never combine.
- Birth control pills/contraceptives: Reduces effectiveness, increasing risk of unintended pregnancy
- Blood thinners (warfarin): Reduces effectiveness, increases clot risk
- HIV medications (protease inhibitors, NNRTIs): Reduces effectiveness, risking treatment failure and viral resistance
- Immunosuppressants (cyclosporine, tacrolimus): Reduces effectiveness — a 2000 case report documented acute heart transplant rejection caused by this interaction
- Cancer medications (imatinib, irinotecan): Reduces effectiveness
- Heart medications (digoxin, statins): Alters blood levels
- Migraine medications (triptans): Risk of serotonin syndrome
The bottom line: If you take any prescription medication, avoid St. John's wort entirely. And if you've been taking it and need to start a prescription drug, know that it takes 2–4 weeks after stopping St. John's wort for enzyme activity to return to normal.
How Does Vitamin K Interact with Warfarin and Other Blood Thinners?
Warfarin (Coumadin) works by blocking the production of vitamin K-dependent clotting factors (II, VII, IX, and X). Vitamin K directly opposes this mechanism — it promotes the production of those same clotting factors. Eating more vitamin K lowers your INR (international normalized ratio), putting you at higher risk for blood clots. Eating less raises your INR, increasing bleeding risk.
The key recommendation is not to avoid vitamin K foods — that would deprive you of essential nutrition from leafy greens. Instead, maintain a consistent vitamin K intake week to week. Target approximately 90–120 mcg daily. Don't take vitamin K supplements unless directed by your doctor. Monitor INR regularly.
High vitamin K foods include kale, spinach, collard greens, broccoli, Brussels sprouts, and green tea. You can absolutely eat these — just keep your portions relatively stable from week to week. Avoid sudden large swings in intake.
Newer anticoagulants (apixaban/Eliquis, rivaroxaban/Xarelto, dabigatran/Pradaxa) are less affected by dietary vitamin K, but you should still avoid vitamin K supplements while taking them.
How Do Mineral Supplements Interfere with Antibiotics?
Calcium, iron, magnesium, and zinc form insoluble chelation complexes with fluoroquinolone antibiotics (ciprofloxacin, levofloxacin, moxifloxacin) and tetracycline antibiotics (doxycycline, minocycline). These complexes cannot be absorbed, reducing antibiotic bioavailability by up to 40% — which can mean the difference between clearing an infection and treatment failure.
The rule is simple but critical: separate all mineral supplements from these antibiotics by at least 2 hours — preferably 4–6 hours. Take antibiotics on an empty stomach when possible, and take your minerals with meals at a different time of day. This interaction also applies to mineral-containing antacids and multivitamins.
Why Must You Separate Supplements from Thyroid Medication?
Levothyroxine (Synthroid, Levoxyl) is notoriously sensitive to absorption interference. Calcium, iron, and magnesium all bind to levothyroxine in the gut, reducing its absorption and potentially worsening hypothyroid symptoms or requiring dose adjustments.
The standard guidance: take thyroid medication on an empty stomach, 30–60 minutes before breakfast, and separate it from all supplements by at least 4 hours. This means taking your supplements with lunch, dinner, or before bed — not with your morning thyroid dose.
What Other Drug-Supplement Combinations Increase Bleeding Risk?
Fish oil, vitamin E, garlic supplements, and ginkgo biloba all have mild blood-thinning effects. Combined with anticoagulant medications (warfarin, apixaban, rivaroxaban), they can increase bleeding risk. If you take blood thinners, avoid high doses of these supplements or use them only under medical supervision. Stop blood-thinning supplements 1–2 weeks before any scheduled surgery.
Additionally, vitamin D and calcium combined with thiazide diuretics (hydrochlorothiazide) can cause dangerously high blood calcium levels. And potassium supplements combined with ACE inhibitors (lisinopril), ARBs (losartan), or potassium-sparing diuretics (spironolactone) can cause hyperkalemia — a potentially fatal heart rhythm disturbance.
How Do You Space Your Supplements to Avoid Harmful Interactions?
The most practical way to prevent supplement interactions is creating a daily timing schedule that separates competing nutrients by at least 2 hours. Group compatible supplements together, isolate problem combinations, and always take thyroid medication and antibiotics far from any mineral supplement. A pill organizer with morning, midday, and evening compartments makes this system sustainable.
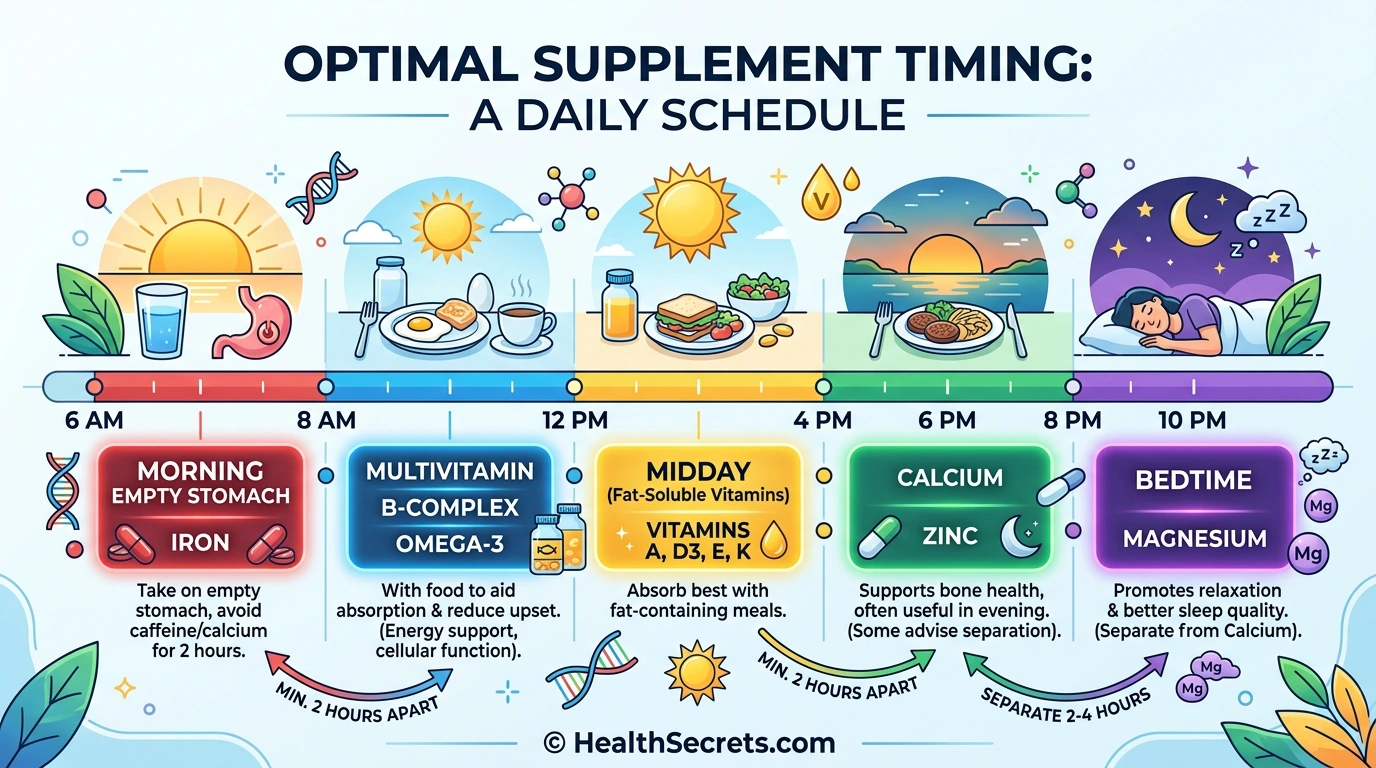
What Should Your Morning Supplement Routine Look Like?
Empty stomach (30–60 min before breakfast):
- Thyroid medication (if applicable) — separate from ALL supplements by 4 hours
- Probiotics (if the product recommends empty stomach)
- Iron with vitamin C — avoid calcium-rich breakfast foods
With breakfast:
- Multivitamin or B-complex
- Vitamin D (with fat-containing meal)
- Omega-3 fish oil
- CoQ10
- Probiotics (if the product recommends with food)
How Should You Distribute Supplements Through the Day?
Midday (with lunch):
- Fat-soluble vitamins (A, E, K) if not taken at breakfast
- Omega-3 fish oil (if splitting the dose)
Afternoon (empty stomach, 2–3 hours after lunch):
- Iron (if not taken in morning) with vitamin C
- Zinc (if taking on empty stomach)
Evening (with dinner):
- Calcium carbonate (requires stomach acid from meal)
- Vitamin K2 (if taking separately)
- Zinc (if taking with food)
Before bed (30–60 minutes):
- Magnesium glycinate or citrate
- Calcium citrate (doesn't require food)
What Are the Essential Spacing Rules to Remember?
| Interaction Pair | Minimum Spacing | Preferred Spacing |
|---|---|---|
| Calcium + Iron | 2 hours | 4 hours |
| Calcium + Zinc | 2 hours | 4 hours |
| Iron + Zinc | 2 hours | 4 hours |
| Minerals + Antibiotics | 2 hours | 4–6 hours |
| ALL supplements + Thyroid meds | 4 hours | 4+ hours |
| Fiber supplements + Everything | 2 hours | 4 hours |
What Diet and Lifestyle Habits Help You Avoid Supplement Interactions?
Maintaining consistent dietary patterns — especially with vitamin K-rich foods — using a pill organizer, keeping an updated supplement-medication list, and scheduling an annual pharmacist interaction review are the most effective lifestyle strategies for preventing supplement interactions. These habits catch problems before they start.
- Keep vitamin K intake consistent. If you take warfarin, the goal isn't to avoid leafy greens — it's to eat roughly the same amount each week. Sudden spikes or drops in kale, spinach, or broccoli consumption will throw off your INR. Create a weekly meal rotation that includes similar servings of green vegetables.
- Avoid grapefruit with certain medications. Grapefruit and grapefruit juice inhibit CYP3A4 in your gut wall, which can dramatically increase blood levels of statins (atorvastatin, simvastatin), calcium channel blockers, benzodiazepines, and immunosuppressants. The effect can last 24+ hours from a single glass. Check your medication labels or ask your pharmacist.
- Use a compartmentalized pill organizer. A weekly pill organizer with AM/PM or morning/midday/evening compartments is the single most practical tool for maintaining proper supplement spacing. Pre-sort your supplements once a week and you won't have to think about timing each day.
- Maintain a master supplement-medication list. Write down every supplement, vitamin, herb, and medication you take — including doses and timing. Bring this list to every doctor's appointment and pharmacy visit. Use free tools like the Drugs.com Interaction Checker to screen for conflicts.
- Schedule a pharmacist review annually. Pharmacists are trained specifically in drug interactions. Most will review your complete supplement and medication list for free. This is especially important if you take blood thinners, thyroid medication, immunosuppressants, or more than 3–4 daily supplements.
Know when to consult your healthcare provider immediately:
- Before starting any supplement if you take prescription medications
- If you experience unusual symptoms after adding a new supplement
- Before any scheduled surgery (stop blood-thinning supplements 1–2 weeks prior)
- If you're pregnant or breastfeeding
- If you have kidney disease, liver disease, or heart conditions

What Should You Do First to Protect Yourself from Supplement Interactions?
Start by auditing your current supplement and medication regimen today. Write down everything you take, check for the major interaction pairs listed below, adjust your timing schedule, and get a pharmacist review within the next two weeks. Prevention is far easier than dealing with the consequences of an undetected interaction.
Phase 1: Immediate Audit (Today)
- List every supplement, vitamin, herb, and medication you currently take
- Check for the major interaction pairs: calcium-iron, zinc-copper, St. John's wort-any medication, vitamin K-warfarin
- Verify you're not taking St. John's wort with any prescription drug
- Check your zinc dose — if above 40 mg, add copper supplementation
Phase 2: Spacing Schedule (This Week)
- Create a daily supplement timing schedule using the spacing rules above
- Get a pill organizer with at least 3 daily compartments (morning, midday, evening)
- Move iron to a separate time from calcium and other minerals
- Ensure thyroid medication is separated from all supplements by 4+ hours
Phase 3: Professional Review (Within 2 Weeks)
- Bring your complete supplement-medication list to your pharmacist
- Ask specifically about interactions between your supplements and any prescriptions
- Use the Drugs.com Interaction Checker as a secondary screen
- Schedule follow-up if any adjustments are needed
Phase 4: Ongoing Maintenance (Monthly)
- Review your regimen whenever you add or remove a supplement
- Monitor for signs of nutrient depletion (fatigue, weakness, easy bruising)
- Keep vitamin K intake consistent if on warfarin
- Get annual bloodwork to check iron, copper, and zinc levels if supplementing




