
Iron deficiency remains the single most prevalent nutritional deficiency on the planet, affecting an estimated 2 billion people and causing iron deficiency anemia in roughly 25% of the global population. For menstruating women, vegetarians, athletes, and pregnant individuals, the risk climbs even higher — yet many people supplement incorrectly, choose the wrong form, or never get tested in the first place.
The challenge with iron is its dual nature: absolutely essential for oxygen transport, energy production, and cognitive function, yet potentially toxic when taken in excess. Unlike most minerals, the human body has no active mechanism to excrete iron — making proper testing, form selection, and dosing critical.
This guide breaks down everything you need to know about iron supplementation — from understanding your lab results and choosing between ferrous sulfate, bisglycinate, and other forms, to optimizing absorption with vitamin C and avoiding common mistakes that sabotage your progress.
This content is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider before starting any supplement regimen, especially iron, which requires testing before use.
What Is Iron and Why Is It Essential for Your Health?
Iron is an essential trace mineral that your body cannot produce on its own — you must obtain it through diet or supplementation. It serves as the core component of hemoglobin, the protein in red blood cells responsible for transporting oxygen from your lungs to every tissue in your body. Adults carry approximately 3–4 grams of total body iron, with about 65% in hemoglobin, 25% in storage proteins (ferritin and hemosiderin), and 10% in muscle myoglobin.
Dietary iron comes in two forms: heme iron from animal sources (meat, poultry, fish) with 15–35% absorption, and non-heme iron from plant sources and supplements with just 2–20% absorption. This dramatic difference in bioavailability is why vegetarians and vegans need approximately 1.8 times more dietary iron than meat-eaters. The body tightly regulates iron absorption through hepcidin, a liver hormone that acts as the master iron regulator — increasing when stores are adequate and decreasing when the body needs more iron.
What Are the Two Types of Dietary Iron?
Heme iron is bound to hemoglobin and myoglobin in animal tissues and absorbs at 15–35% regardless of other dietary factors.
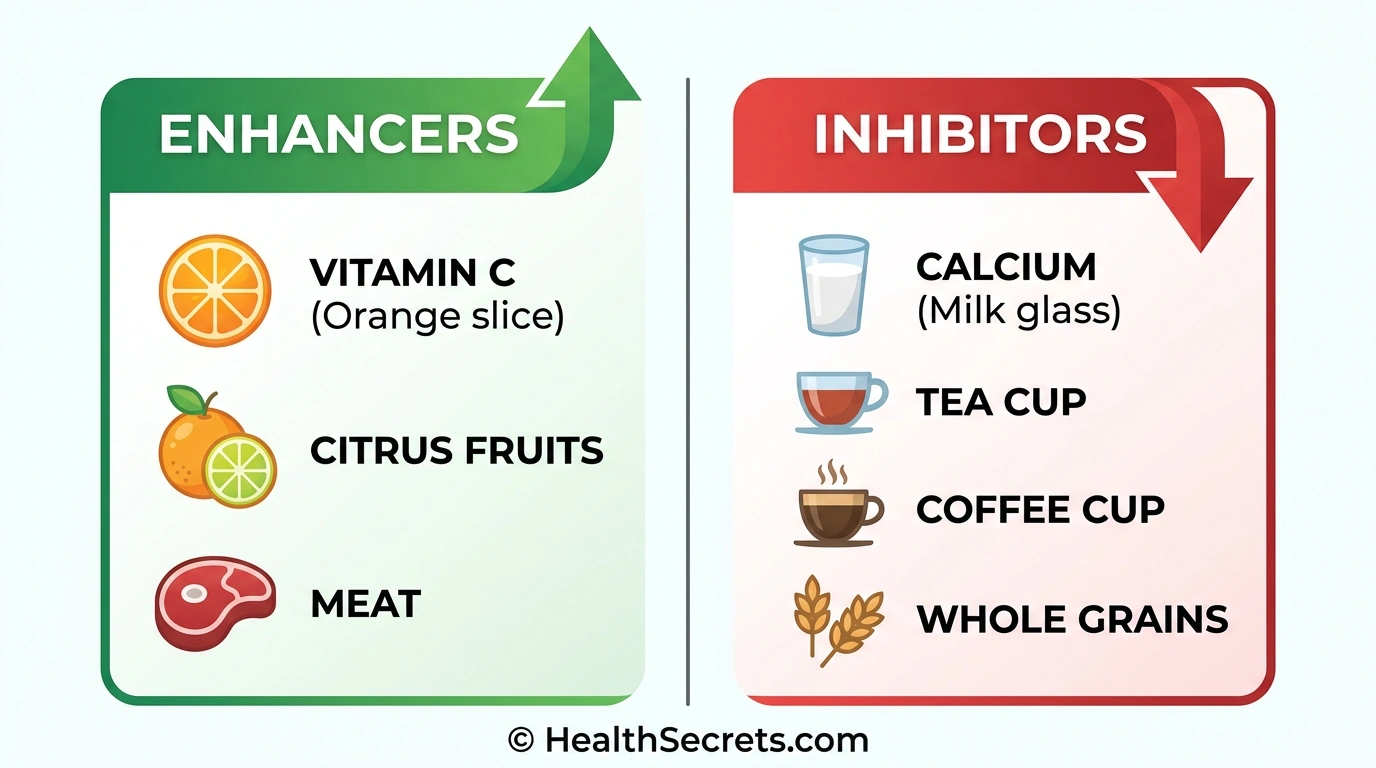
Non-heme iron is the free form found in plants, fortified foods, and all supplements — it absorbs at just 2–20% and is heavily influenced by enhancers (vitamin C) and inhibitors (calcium, tannins, phytates). All oral iron supplements deliver non-heme iron, which is why absorption optimization matters so much.
How Is Iron Distributed in Your Body?
Your body distributes iron across four major compartments: hemoglobin (65%) in red blood cells for oxygen transport, ferritin and hemosiderin (25%) as storage in the liver, spleen, and bone marrow, myoglobin (10%) in muscles for local oxygen storage, and enzymes (<1%) for metabolic functions including DNA synthesis, detoxification, and energy production. The body efficiently recycles approximately 90% of iron from old red blood cells through a process managed by macrophages in the spleen.
How Does Iron Work in Your Body?
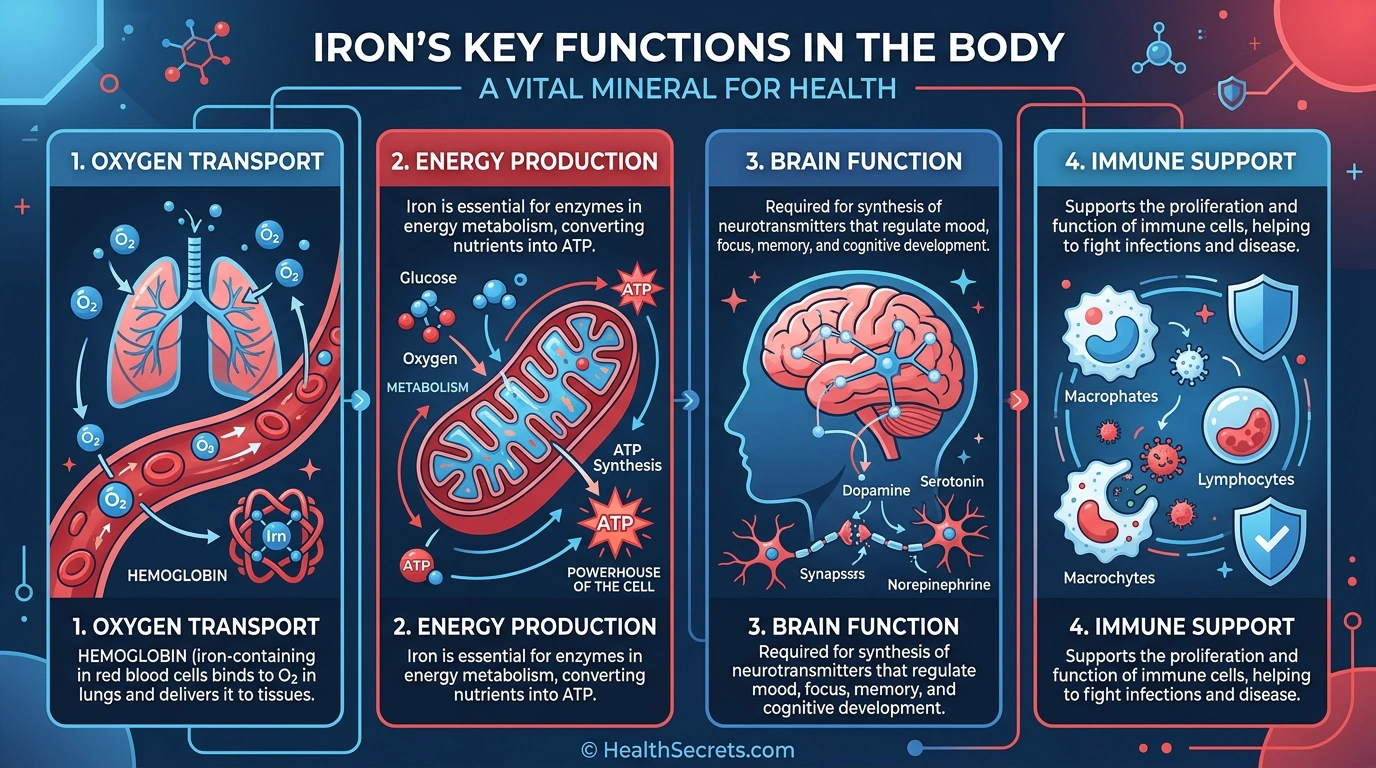
Iron performs several critical biological functions beyond oxygen transport. Understanding these mechanisms explains why even mild deficiency — before anemia develops — can cause fatigue, brain fog, and impaired immunity. Iron's roles span from cellular energy production to neurotransmitter synthesis.
How Does Iron Transport Oxygen Throughout Your Body?
Iron sits at the center of hemoglobin's heme group, where it binds oxygen molecules in the lungs and releases them in tissues. Each hemoglobin molecule contains four iron atoms, enabling each red blood cell to carry approximately 1 billion oxygen molecules. When iron stores drop, hemoglobin production decreases, oxygen delivery becomes inefficient, and tissues experience hypoxia — manifesting as fatigue, shortness of breath, and exercise intolerance. Myoglobin, a related iron-containing protein in muscle cells, stores oxygen locally for immediate use during physical activity.
Why Does Iron Deficiency Cause Fatigue Even Without Anemia?
Iron is a required cofactor in the mitochondrial electron transport chain, specifically in cytochrome enzymes that produce ATP — your body's primary energy currency. Research published in the American Journal of Clinical Nutrition demonstrated that iron supplementation significantly improved fatigue scores and quality of life in iron-deficient women who were not yet anemic, confirming that depleted iron stores impair energy production before hemoglobin drops below the anemia threshold.
How Does Iron Affect Brain Function and Mood?
Iron is essential for synthesizing dopamine, serotonin, and norepinephrine — neurotransmitters that regulate mood, motivation, and cognitive performance. It also supports myelin formation, the insulating sheath around nerve fibers that enables rapid signal transmission. Studies in adolescents have shown that iron supplementation improved memory, attention, and learning capacity in those with low ferritin levels. Iron deficiency during infancy and early childhood can cause irreversible cognitive developmental delays.
Does Iron Support Immune Function?
Iron is required for the proliferation and maturation of immune cells, particularly lymphocytes and neutrophils. However, iron regulation in immunity involves a delicate balance — while deficiency impairs immune response and increases infection susceptibility, excess iron can actually feed pathogenic bacteria and parasites. This is why the body sequesters iron during acute infections through hepcidin upregulation, a process called "nutritional immunity."
How Well Are Different Iron Supplements Absorbed?
Iron supplement absorption varies dramatically depending on the chemical form, what you take it with, and your current iron status. Choosing the right form and optimizing absorption conditions can mean the difference between effective repletion and months of frustration with no improvement.
Ferrous vs. ferric forms: Ferrous (Fe²⁺) iron is significantly better absorbed than ferric (Fe³⁺) iron because the intestinal transporter DMT1 preferentially absorbs the ferrous form. Ferric iron must first be reduced to ferrous iron by stomach acid and duodenal cytochrome b before absorption — an extra step that reduces bioavailability.
:::info[Iron forms comparison:]
| Form | Elemental Iron | Absorption | GI Tolerance | Best For |
|---|---|---|---|---|
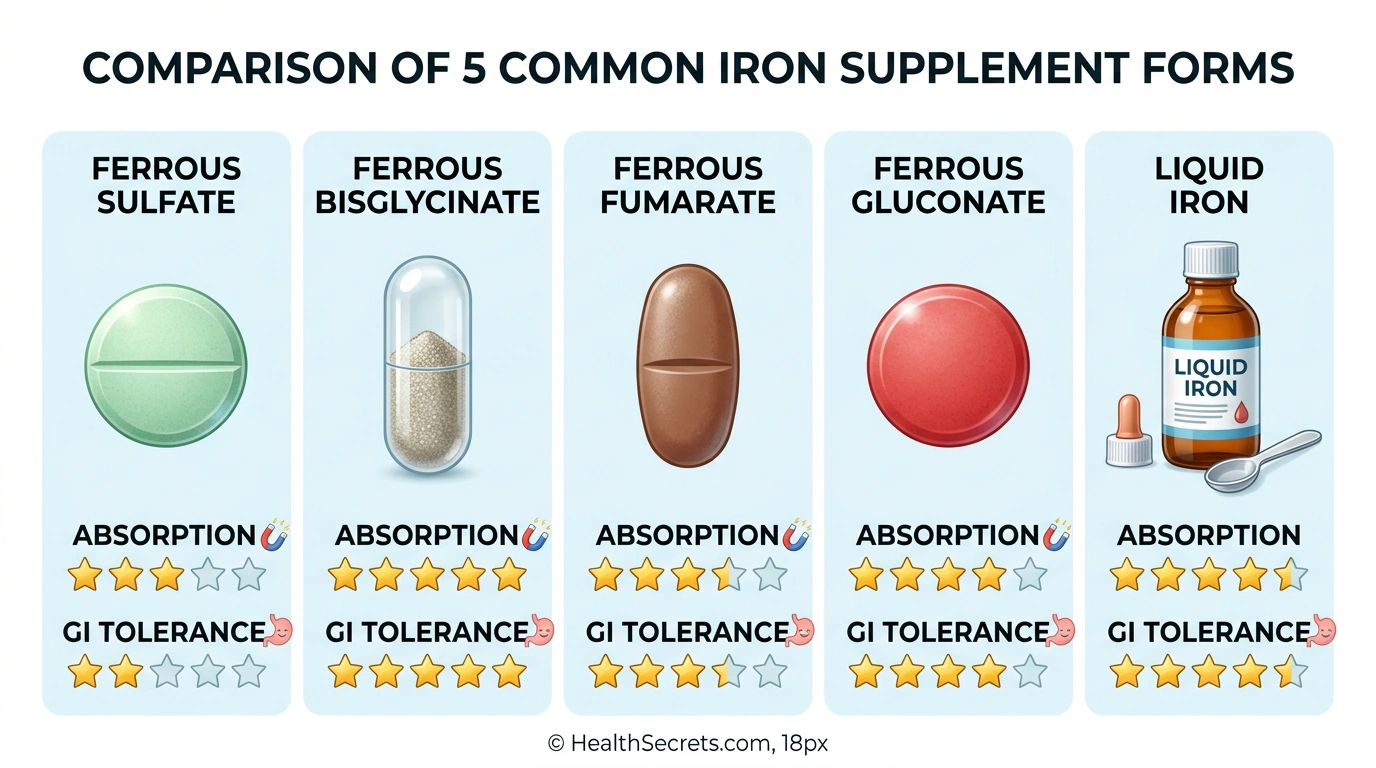
| Ferrous Sulfate | 20% (65 mg/325 mg) | Good | Poor | Budget, severe deficiency |
| Ferrous Bisglycinate | ~20% (25–50 mg/cap) | Excellent | Excellent | GI sensitivity, first choice |
| Ferrous Fumarate | 33% (106 mg/325 mg) | Good | Poor–Moderate | High elemental iron needs |
| Ferrous Gluconate | 12% (38 mg/325 mg) | Good | Moderate | Moderate deficiency |
| Carbonyl Iron | ~99% pure | Moderate (slow) | Good | Safety-focused, children |
| ::: |
Ferrous bisglycinate deserves special attention: a randomized trial published in the Journal of Perinatal Medicine found that 25 mg of iron as bisglycinate was as effective as 50 mg of ferrous sulfate for preventing iron deficiency during pregnancy, with significantly fewer GI complaints (P=0.001). The chelated glycine molecules protect iron through the stomach and enhance absorption through a separate amino acid transport pathway.
Key absorption enhancers and inhibitors:
- Vitamin C (ascorbic acid): The most powerful enhancer — increases non-heme iron absorption 3–4x by reducing Fe³⁺ to Fe²⁺ and forming soluble chelates. Take 100–200 mg with your iron supplement.
- Calcium: Strongly inhibits absorption. Separate dairy and calcium supplements by at least 2 hours.
- Tannins (tea and coffee): Can reduce absorption by 50–90%. Avoid within 1–2 hours of iron.
- Phytates: Found in whole grains, legumes, and nuts. Soaking and sprouting reduces phytate content.
- PPIs and antacids: Reduce stomach acid needed for iron absorption. Separate by 2–4 hours.
Alternate-day dosing: Groundbreaking research from ETH Zurich demonstrated that iron absorption was significantly higher (+33%) with alternate-day dosing compared to consecutive-day dosing. Oral iron triggers a hepcidin spike that persists for 24 hours, temporarily blocking further absorption. This finding suggests that taking iron every other day may be more effective than daily dosing for many people.
How Much Iron Should You Take Daily?
Iron dosing depends on your current status, the reason for supplementation, and which form you choose. The critical distinction is between elemental iron (the actual iron your body absorbs) and total compound weight — a 325 mg ferrous sulfate tablet contains only 65 mg of elemental iron. Always dose based on elemental iron content.
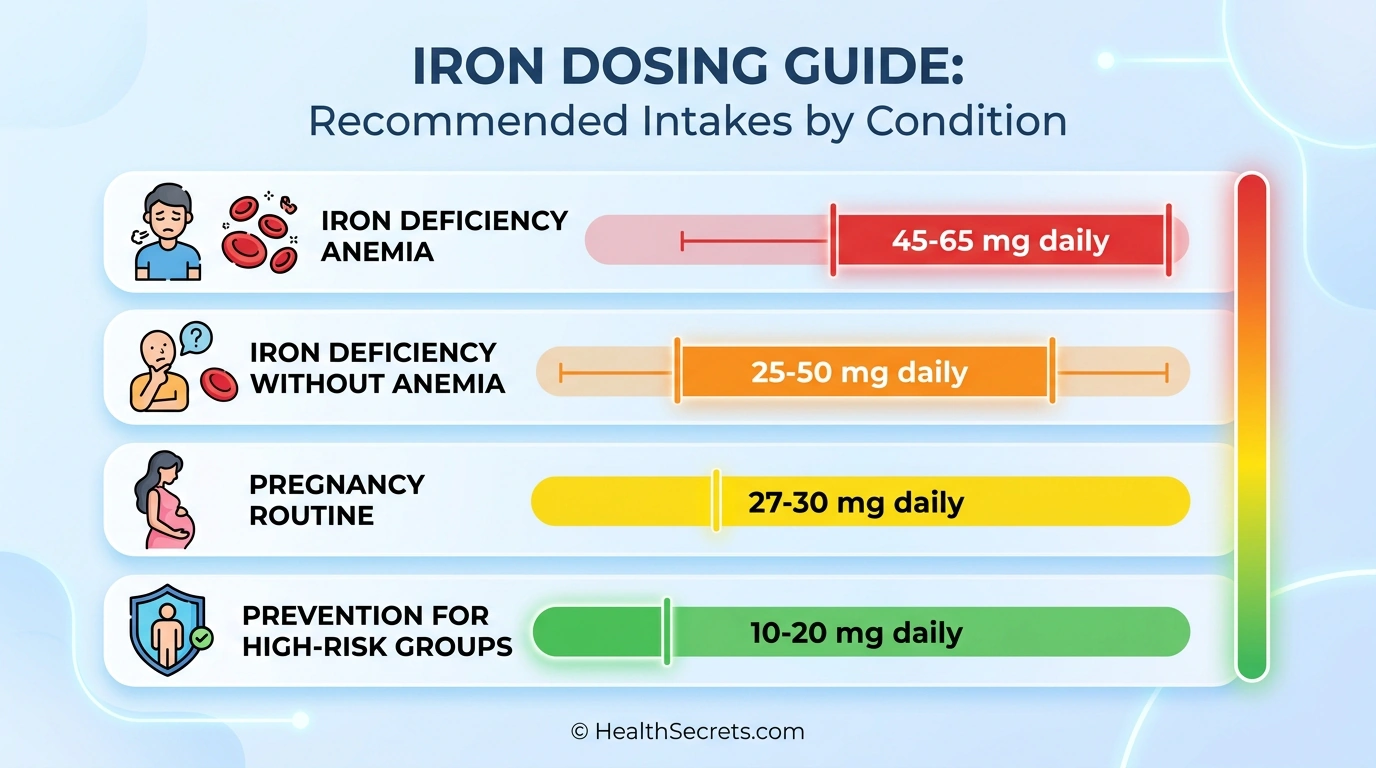
| Condition | Elemental Iron | Duration | Preferred Form |
|---|---|---|---|
| Iron deficiency (no anemia) | 25–50 mg/day | 3–6 months, retest | Bisglycinate |
| Iron deficiency anemia | 45–65 mg/day | 3–6 months minimum | Sulfate or bisglycinate |
| Pregnancy (routine) | 27–30 mg/day | Throughout pregnancy | Bisglycinate preferred |
| Pregnancy (anemic) | 60–120 mg/day | Medical supervision | Bisglycinate or sulfate |
| Prevention (high-risk) | 10–20 mg/day | Ongoing while at risk | Low-dose bisglycinate |
| Important dosing principles: |
- Start low, go slow: Begin with a lower dose and increase as tolerated to minimize GI side effects
- Divide large doses: If taking >65 mg elemental iron, split into two doses for better absorption and fewer side effects
- Empty stomach vs. with food: Empty stomach maximizes absorption (2–3x better) but causes more GI upset. Take with a small, low-calcium meal if intolerant
- Tolerable Upper Intake Level: 45 mg elemental iron/day from supplements. Therapeutic doses for anemia exceed this and require medical supervision
- Retest at 3 months: Check ferritin and hemoglobin to assess progress and adjust dosing
- Don't stop too early: Continue supplementation until ferritin reaches >50 ng/mL, even if hemoglobin normalizes first — stores take longer to replenish
Thorne Iron Bisglycinate
Editor's ChoiceThorne Iron · Overall best iron supplement — excellent absorption with minimal side effects
Nature Made Iron 65 mg
Best BudgetNature Made · Affordable, effective iron for confirmed deficiency or anemia
Solgar Gentle Iron 25 mg
Best Gentle IronSolgar Gentle · Sensitive stomachs and those who failed ferrous sulfate due to GI issues
MegaFood Blood Builder
Best Iron + Vitamin C CombinationMegaFood Blood · Comprehensive iron support with built-in absorption enhancers
Flora Floradix Liquid Iron + Herbs
Best Liquid IronFlora Floradix · People who cannot swallow pills or prefer liquid supplementation
Garden of Life Vitamin Code Raw Iron
Best Whole Food IronGarden of · Those preferring whole-food-based supplements with comprehensive nutrient support
NOW Foods Iron 36 mg Double Strength
Best Value BisglycinateNOW Foods · Higher-dose bisglycinate at an affordable price point
Vitron-C High Potency Iron + Vitamin C
Best Iron + C Combo (Budget)Vitron-C High · Convenient iron plus vitamin C in a single, affordable tablet
Three Arrows Heme Iron Supplement
Best Heme IronThree Arrows · Maximum absorption without dietary inhibitor concerns
Read the detailed review cards below before opening any retailer link
Top Recommended Products

Thorne Iron
Thorne Iron Bisglycinate
Thorne's iron bisglycinate delivers the most well-tolerated form of supplemental iron with excellent absorption, backed by NSF certification that guarantees purity and potency — ideal for long-term supplementation.
Pros
- + Best-in-class tolerability
- + NSF Certified for Sport
- + no common allergens
- + well-researched form
Cons
- - Lower elemental iron per capsule (may need 2 for severe deficiency)
- - premium price vs ferrous sulfate
Why we included it: Thorne's iron bisglycinate delivers the most well-tolerated form of supplemental iron with excellent absorption, backed by NSF certification that guarantees purity and potency — ideal for long-term supplementation.
Retailer link opens on Amazon after the review details above

Nature Made
Nature Made Iron 65 mg
Nature Made's USP-verified ferrous sulfate is the gold standard for treating iron deficiency anemia on a budget — the same form used in most clinical trials demonstrating efficacy.
Pros
- + USP Verified for purity and potency
- + lowest cost per dose
- + high elemental iron
- + most studied form
Cons
- - Higher GI side effect risk (constipation
- - nausea)
- - may need to take with food
- - metallic taste possible
Why we included it: Nature Made's USP-verified ferrous sulfate is the gold standard for treating iron deficiency anemia on a budget — the same form used in most clinical trials demonstrating efficacy.
Retailer link opens on Amazon after the review details above

Solgar Gentle
Solgar Gentle Iron 25 mg
Solgar Gentle Iron is specifically formulated for people who experience constipation, nausea, or stomach upset from traditional iron supplements — the bisglycinate chelate form virtually eliminates GI complaints.
Pros
- + Extremely gentle on stomach
- + suitable for vegetarians
- + multiple certifications
- + no metallic taste
Cons
- - Lower dose requires 2 capsules for higher needs
- - slightly more expensive than sulfate
Why we included it: Solgar Gentle Iron is specifically formulated for people who experience constipation, nausea, or stomach upset from traditional iron supplements — the bisglycinate chelate form virtually eliminates GI complaints.
Retailer link opens on Amazon after the review details above

MegaFood Blood
MegaFood Blood Builder
MegaFood Blood Builder is clinically shown to increase iron levels without common side effects, combining iron bisglycinate with synergistic nutrients (folate, B12, vitamin C) for a complete blood-building formula.
Pros
- + Clinically studied formula
- + includes vitamin C
- + folate
- + and B12 for comprehensive blood building
- + gentle
- + vegan
Cons
- - Premium pricing
- - lower vitamin C than ideal (consider adding more)
- - larger tablet size
Why we included it: MegaFood Blood Builder is clinically shown to increase iron levels without common side effects, combining iron bisglycinate with synergistic nutrients (folate, B12, vitamin C) for a complete blood-building formula.
Retailer link opens on Amazon after the review details above

Flora Floradix
Flora Floradix Liquid Iron + Herbs
Floradix has been the world's bestselling liquid iron supplement for decades, combining gentle ferrous gluconate with vitamin C and herbal extracts in a format ideal for those who struggle with capsules or tablets.
Pros
- + Easy to absorb liquid form
- + includes vitamin C and B vitamins
- + pleasant taste
- + gentle on stomach
Cons
- - Must be refrigerated after opening
- - lower iron per dose (10 mg)
- - shorter shelf life
- - higher cost per mg
Why we included it: Floradix has been the world's bestselling liquid iron supplement for decades, combining gentle ferrous gluconate with vitamin C and herbal extracts in a format ideal for those who struggle with capsules or tablets.
Retailer link opens on Amazon after the review details above

Garden of
Garden of Life Vitamin Code Raw Iron
Garden of Life combines whole-food iron with probiotics and digestive enzymes, making it an excellent choice for those who want comprehensive nutritional support and gentle digestion alongside iron repletion.
Pros
- + Whole food nutrients
- + includes probiotics for GI support
- + gentle
- + vegan
- + comprehensive formula
Cons
- - Only 30 capsules per bottle
- - premium price per serving
- - lower iron dose for severe deficiency
Why we included it: Garden of Life combines whole-food iron with probiotics and digestive enzymes, making it an excellent choice for those who want comprehensive nutritional support and gentle digestion alongside iron repletion.
Retailer link opens on Amazon after the review details above

NOW Foods
NOW Foods Iron 36 mg Double Strength
NOW Foods delivers a higher-dose bisglycinate using the patented Ferrochel chelate from Albion Minerals at a fraction of premium brand pricing — excellent value for those needing more than 25 mg per dose.
Pros
- + Higher dose bisglycinate (36 mg) at competitive price
- + Ferrochel branded chelate
- + gentle
- + vegan
Cons
- - May be more than needed for prevention
- - no added vitamin C (take separately)
Why we included it: NOW Foods delivers a higher-dose bisglycinate using the patented Ferrochel chelate from Albion Minerals at a fraction of premium brand pricing — excellent value for those needing more than 25 mg per dose.
Retailer link opens on Amazon after the review details above

Vitron-C High
Vitron-C High Potency Iron + Vitamin C
Vitron-C combines the safety advantages of carbonyl iron with built-in vitamin C for absorption enhancement — a smart budget pick, especially for households with children where accidental ingestion safety matters.
Pros
- + Built-in vitamin C for enhanced absorption
- + carbonyl iron is safer in accidental overdose
- + affordable
Cons
- - Carbonyl iron absorbs more slowly than ferrous forms
- - may need longer supplementation
- - fewer third-party certs
Why we included it: Vitron-C combines the safety advantages of carbonyl iron with built-in vitamin C for absorption enhancement — a smart budget pick, especially for households with children where accidental ingestion safety matters.
Retailer link opens on Amazon after the review details above
Three Arrows
Three Arrows Heme Iron Supplement
Heme iron polypeptide mimics the highly bioavailable iron found naturally in meat, absorbing through a separate pathway unaffected by common dietary inhibitors — ideal for those who need maximum absorption.
Pros
- + Highest bioavailability (15–35% absorption)
- + not affected by calcium
- + tea
- + or phytates
- + minimal GI side effects
Cons
- - Animal-derived (not for vegetarians/vegans)
- - premium pricing
- - lower elemental iron per capsule
- - limited availability
Why we included it: Heme iron polypeptide mimics the highly bioavailable iron found naturally in meat, absorbing through a separate pathway unaffected by common dietary inhibitors — ideal for those who need maximum absorption.
Retailer link opens on Amazon after the review details above
Can You Get Enough Iron from Food Alone?
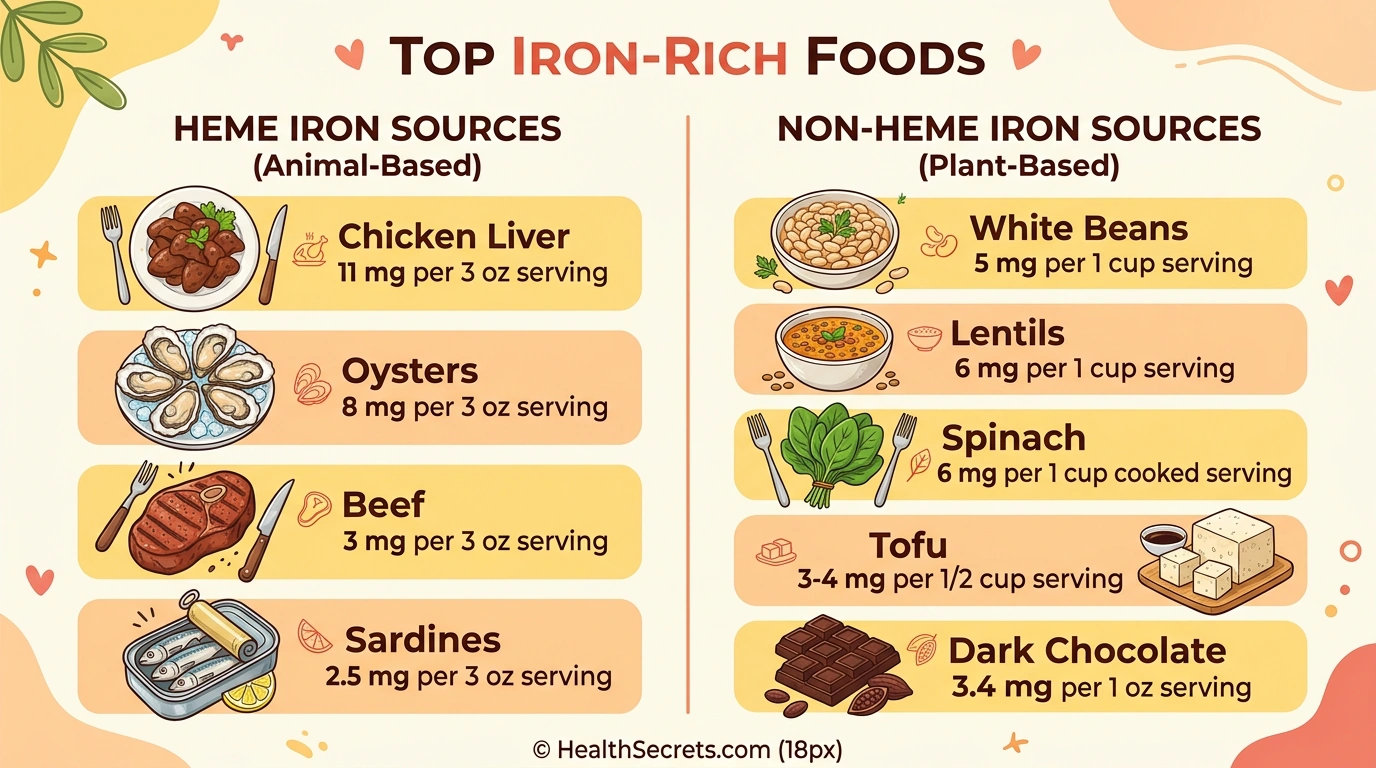
For many people with adequate iron status, a well-planned diet provides sufficient iron — but for those with increased needs or existing deficiency, food alone often falls short. The key difference lies in absorption: heme iron from animal sources is absorbed at 15–35% regardless of other dietary factors, while non-heme iron from plants absorbs at just 2–20% and is heavily influenced by enhancers and inhibitors.
Top iron-rich foods:
| Food | Serving | Iron (mg) | % DV (women) | Type |
|---|---|---|---|---|
| Chicken liver | 3 oz | 11.0 | 61% | Heme |
| Oysters | 3 oz | 8.0 | 44% | Heme |
| White beans | 1 cup | 8.0 | 44% | Non-heme |
| Lentils (cooked) | 1 cup | 6.6 | 37% | Non-heme |
| Spinach (cooked) | 1 cup | 6.4 | 36% | Non-heme |
| Practical tips for boosting dietary iron: Pair plant-based iron sources with vitamin C-rich foods like citrus, bell peppers, or tomatoes. Cook in cast iron cookware — studies show this can increase iron content of acidic foods significantly. Soak legumes and grains before cooking to reduce phytate content and improve mineral availability. Avoid drinking tea or coffee with iron-rich meals. |
For vegetarians, vegans, menstruating women with heavy periods, and athletes — food alone may not be enough to maintain optimal ferritin levels (>50 ng/mL), and targeted supplementation becomes necessary.
Is Iron Supplementation Safe?
Iron supplementation is generally safe when taken at appropriate doses based on confirmed deficiency, but it carries unique risks compared to most supplements because the body lacks an active excretion mechanism for excess iron. This makes testing essential before and during supplementation.
Common side effects and management:
- Constipation (most common): Increase water and fiber intake, consider adding magnesium (300–400 mg has a natural laxative effect), or switch to bisglycinate
- Nausea and stomach upset: Take with a small amount of food, reduce dose, or switch to bisglycinate
- Dark/black stools: Normal and harmless — simply unabsorbed iron. Not to be confused with GI bleeding
- Metallic taste: Switch to bisglycinate (neutral taste) or take with juice
Serious risks:
- Iron overload (hemochromatosis): Genetic condition affecting ~1 in 200 people of Northern European descent. Excess iron deposits in organs causing liver damage, joint pain, diabetes, and heart problems.
Never supplement without testing.
- Acute toxicity: Doses >20 mg/kg body weight can be fatal, especially in children. Keep all iron supplements in child-proof containers and out of reach.
- Drug interactions: Iron reduces absorption of thyroid medications (levothyroxine), certain antibiotics (tetracyclines, fluoroquinolones), and Parkinson's medications (levodopa). Separate by at least 2 hours.
Who should NOT supplement iron without medical guidance:
- Men (low deficiency risk, higher overload risk)
- Postmenopausal women (reduced needs)
- Anyone with hemochromatosis or a family history
- People with chronic infections (iron can feed pathogens)
- Those with inflammatory conditions (ferritin may be falsely elevated)
What Can Iron Supplements Actually Do for You?
Iron supplementation is highly effective for correcting confirmed deficiency and anemia — but setting realistic expectations about timeline, limitations, and individual variation helps you stay consistent and avoid frustration.
Realistic timeline:
- 1–2 weeks: Some people notice improved energy, especially if severely deficient
- 4–8 weeks: Hemoglobin levels typically begin rising (expect ~1–2 g/dL increase)
- 3 months: Significant improvement in hemoglobin; retest ferritin and adjust dose
- 3–6 months: Full iron store repletion (ferritin >50 ng/mL) — this is when you can consider reducing or stopping
- 6–12 months: Some people with severe depletion or ongoing losses need longer supplementation
What iron supplements will NOT do:
- Boost energy if you're not actually iron deficient (fatigue has many causes)
- Work immediately — iron repletion is a gradual process
- Replace the need to address underlying causes (heavy periods, GI bleeding, malabsorption)
- Compensate for a very poor diet long-term without dietary improvements
Individual variation matters: Absorption varies significantly based on your current iron status (depleted bodies absorb more), gut health, concurrent medications, and genetics. If oral supplementation fails to raise ferritin after 3 months of consistent use, discuss IV iron with your healthcare provider — conditions like celiac disease, inflammatory bowel disease, or H. pylori infection may impair oral absorption.
What Should You Do First if You Suspect Iron Deficiency?
If you're experiencing fatigue, brain fog, hair loss, or other deficiency symptoms, following a systematic approach ensures safe and effective iron repletion. Never start iron supplementation without first confirming deficiency through blood testing.
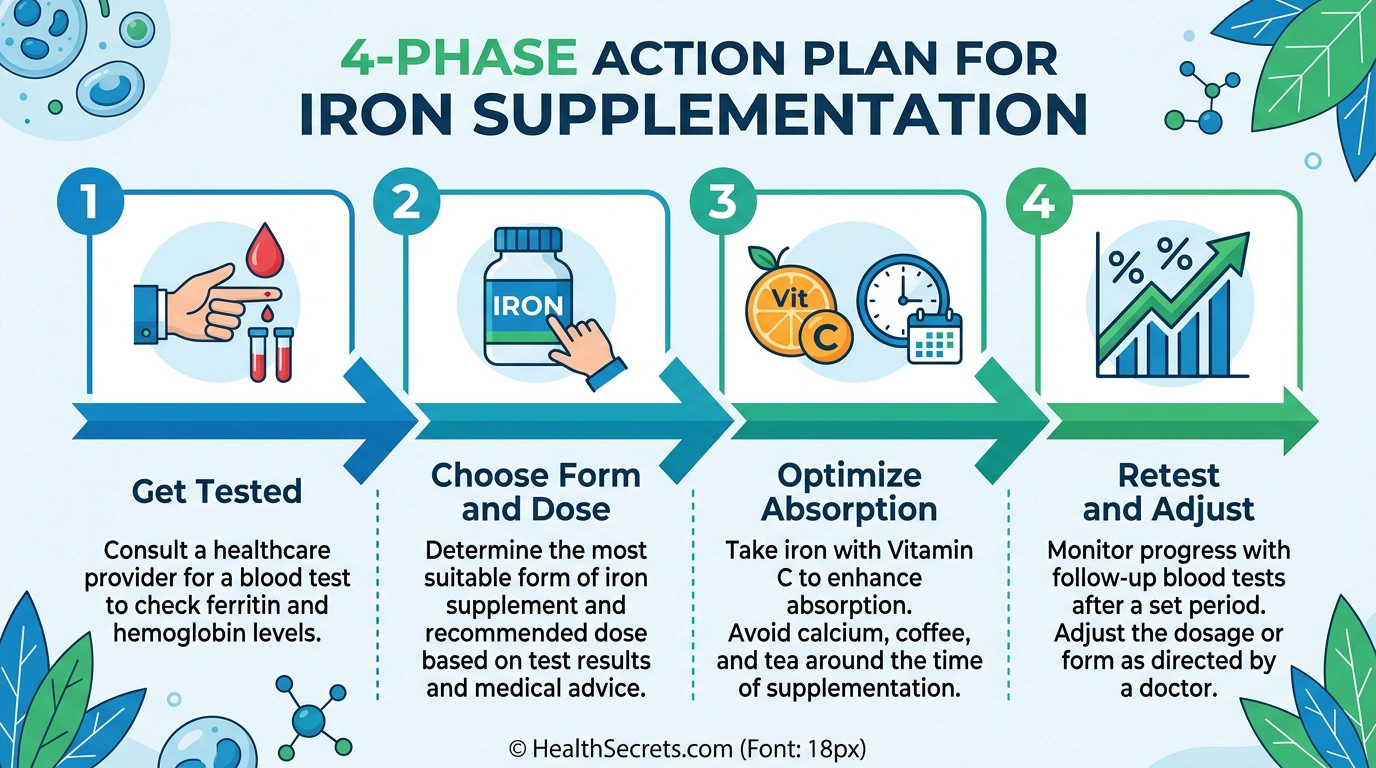
Phase 1 — Get Tested (Week 1):
- Request a complete iron panel: ferritin, serum iron, TIBC, transferrin saturation, hemoglobin/CBC
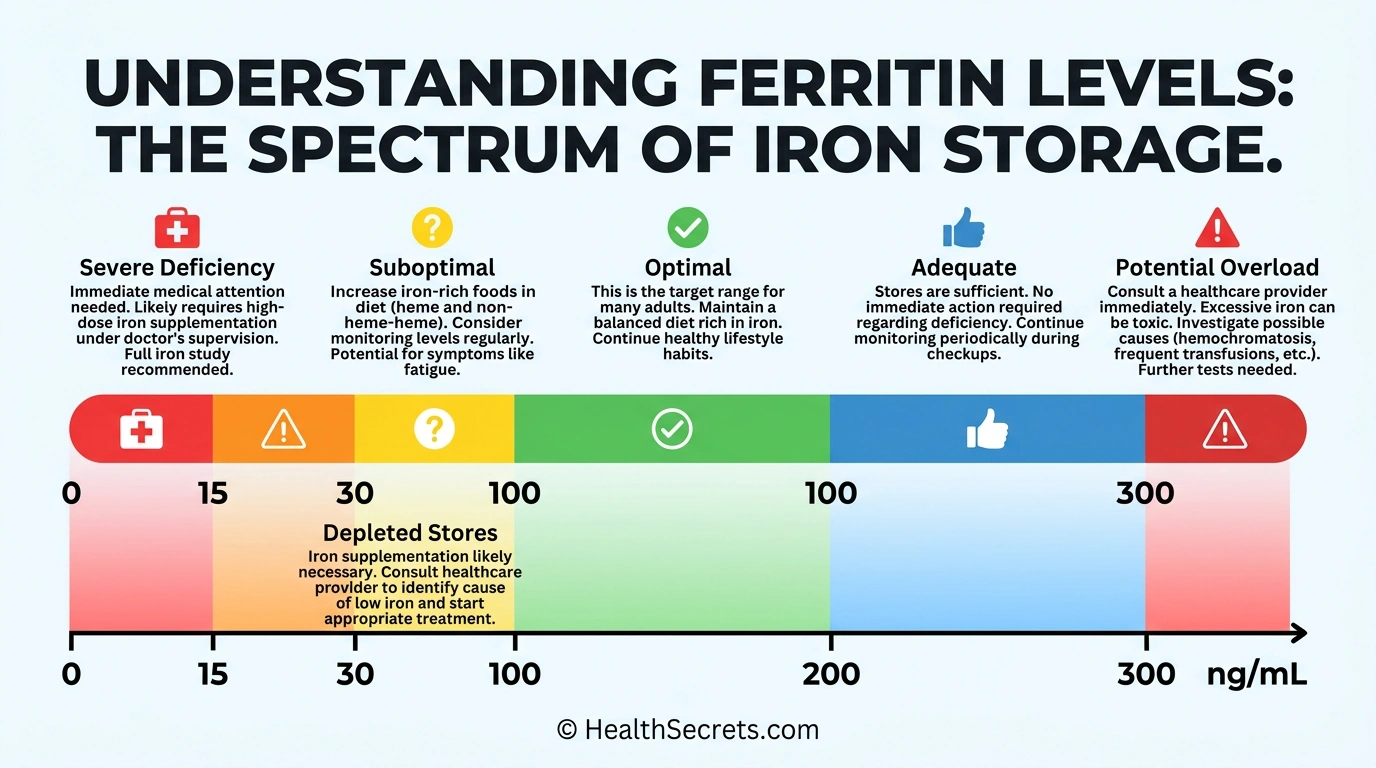
- Ferritin is the single most important marker — optimal is 50–100 ng/mL
- Note: ferritin can be falsely elevated by inflammation or infection
Phase 2 — Choose Your Form and Dose (Week 1–2):
- First choice: ferrous bisglycinate 25–50 mg elemental iron (best tolerated)
- Budget option: ferrous sulfate 325 mg (65 mg elemental iron)
- Purchase vitamin C (100–200 mg) to take alongside iron
- Set a consistent schedule — morning on empty stomach or with light meal
Phase 3 — Optimize and Manage (Weeks 2–12):
- Take iron with vitamin C, away from calcium, tea, and coffee
- Consider alternate-day dosing for better absorption and fewer side effects
- Address constipation early: hydration, fiber, magnesium if needed
- Track symptoms weekly to gauge improvement
Phase 4 — Retest and Adjust (Month 3):
- Recheck ferritin, hemoglobin, and complete iron panel
- If ferritin rising: continue until >50 ng/mL, then reassess
- If no improvement: consult healthcare provider about dose adjustment, form change, or IV iron
- Continue supplementation 3–6 months after hemoglobin normalizes to fully replenish stores




