 Pin It
Pin It Celiac Disease vs Gluten Sensitivity: Complete Guide
Who This Is For
Best for readers who want a grounded introduction to gut health.
Who Should Be Careful
Not for emergency decisions or personalized treatment planning.
Affiliate Disclaimer | This article may contain affiliate links to products we trust. If you choose to buy through them, we may earn a small commission at no extra cost to you. Full disclosure
Medical Disclaimer | For informational purposes only. Not a substitute for professional medical advice. Read full disclaimer
Key Takeaways
Garden of Life Vitamin Code Raw Iron
Best OverallGarden of · Iron-deficiency anemia common in celiac disease
Thorne Zinc Picolinate 30mg
Best for Zinc DeficiencyThorne Zinc · Replenishing zinc stores depleted by celiac malabsorption
NOW Foods L-Glutamine Powder 1lb
Best for Gut HealingNOW Foods · Supporting intestinal barrier repair after celiac diagnosis
Vital Proteins Collagen Peptides 20oz
Best ValueVital Proteins · Comprehensive gut lining and connective tissue support
Read the detailed review cards below before opening any retailer link
If you feel terrible every time you eat bread, pasta, or cereal, you're probably wondering what's actually going on inside your body. Is it celiac disease? Gluten sensitivity? A wheat allergy? The answer matters more than you might think — because each condition involves different immune mechanisms, carries different health risks, and requires a different approach to treatment.
Here's the problem: celiac disease and non-celiac gluten sensitivity can produce nearly identical symptoms. Bloating, fatigue, brain fog, joint pain — the overlap makes self-diagnosis unreliable and potentially dangerous. An estimated 80% of people with celiac disease remain undiagnosed in the United States, which means millions of people may be unknowingly damaging their small intestines.
If you're exploring digestive health, you may also find our guides on gut health fundamentals, healing leaky gut syndrome, and gut-healing foods helpful as companion reading.
What Are Celiac Disease and Gluten Sensitivity, and Why Does It Matter to Know the Difference?
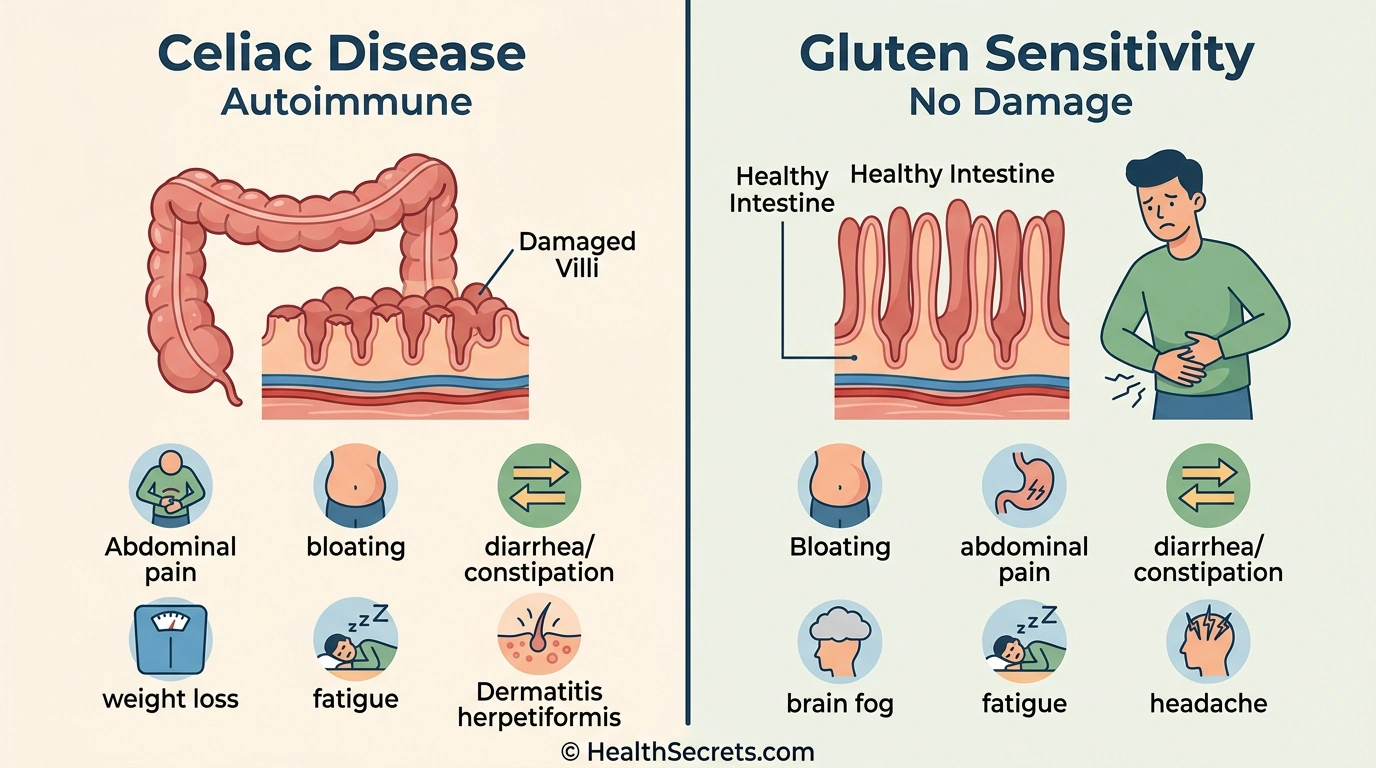
Celiac disease is an autoimmune disorder where gluten triggers the immune system to attack the small intestine, while non-celiac gluten sensitivity (NCGS) causes similar symptoms without autoimmune damage. Accurate differentiation matters because celiac disease carries serious long-term health risks — including malnutrition, osteoporosis, and increased cancer risk — that require strict medical management.
Gluten is a group of storage proteins found in wheat, barley, and rye. It gives bread its chewy texture and helps dough rise. For most people, gluten is perfectly harmless. But for a significant minority, it triggers one of three distinct conditions.
What Is Celiac Disease?
Celiac disease is a hereditary autoimmune disorder affecting approximately 1% of the population worldwide. When someone with celiac disease eats gluten, the immune system produces antibodies — particularly anti-tissue transglutaminase (tTG-IgA) — that attack the villi lining the small intestine. These finger-like projections are responsible for nutrient absorption, and their destruction leads to malabsorption of vitamins, minerals, and macronutrients.
Celiac disease has a strong genetic component. Nearly all people with celiac carry the HLA-DQ2 or HLA-DQ8 genes. However, roughly 30–40% of the general population carries these genes without developing the disease, so genetics alone aren't sufficient for diagnosis.
What Is Non-Celiac Gluten Sensitivity?
NCGS is defined as a symptomatic response to gluten in people who have tested negative for both celiac disease and wheat allergy. Symptoms often overlap significantly with celiac disease — bloating, abdominal pain, fatigue, headaches, and brain fog — but no intestinal damage or autoimmune markers are present.
A 2026 Lancet review found that during controlled challenge studies, only 16–30% of self-reported gluten-sensitive individuals had symptoms specifically triggered by gluten. FODMAPs (fermentable carbohydrates), amylase-trypsin inhibitors (ATIs), and nocebo effects appear to contribute significantly in many cases.
What Is Wheat Allergy?
Wheat allergy is a true IgE-mediated allergic reaction to wheat proteins — not just gluten. It can cause hives, swelling, difficulty breathing, and in severe cases, anaphylaxis. Unlike celiac disease and NCGS, wheat allergy triggers a rapid immune response (within minutes to hours) and is diagnosed through skin prick tests and wheat-specific IgE blood tests.
How Do These Three Conditions Affect Your Body Differently?
Each gluten-related disorder involves a different immune mechanism. Celiac disease triggers an autoimmune response that destroys intestinal villi. NCGS activates the innate immune system without autoimmunity. Wheat allergy produces an IgE-mediated allergic reaction. Understanding these differences is essential for proper treatment.

How Does Celiac Disease Damage the Intestine?
In celiac disease, gluten peptides — particularly gliadin — cross the intestinal barrier and trigger an adaptive immune response. The enzyme tissue transglutaminase modifies gliadin, making it highly immunogenic. T-cells attack the intestinal lining, causing villous atrophy (flattening of the villi), crypt hyperplasia, and chronic inflammation. This damage reduces the absorptive surface area, leading to deficiencies in iron, B12, folate, calcium, vitamin D, and zinc.
What Mechanisms Drive Non-Celiac Gluten Sensitivity?
The exact mechanisms of NCGS remain under investigation. Current research points to innate immune activation rather than the adaptive immune response seen in celiac disease. There's evidence of increased intestinal permeability and mild inflammation, but without the hallmark villous atrophy. Researchers now suspect that wheat components beyond gluten — particularly ATIs and FODMAPs — may be the primary triggers in many patients.
| Feature | Celiac Disease | NCGS | Wheat Allergy |
|---|---|---|---|
| Immune mechanism | Autoimmune (adaptive) | Innate immune activation | IgE-mediated allergy |
| Intestinal damage | Yes (villous atrophy) | No (or minimal) | No |
| Specific biomarkers | tTG-IgA, EMA-IgA | None currently | Wheat-specific IgE |
| Genetic markers | HLA-DQ2/DQ8 | Not established | Not established |
| Prevalence | ~1% of population | 0.5–13% (uncertain) | 0.2–1% |

What Are the Key Benefits of Getting an Accurate Diagnosis for Gluten-Related Disorders?
An accurate diagnosis determines the right treatment, prevents unnecessary dietary restrictions, and identifies serious health risks early. People with undiagnosed celiac disease face progressive intestinal damage, while those misdiagnosed with celiac may follow unnecessarily strict diets that reduce quality of life and nutritional adequacy.

Does Early Celiac Diagnosis Prevent Long-Term Complications?
Yes. Undiagnosed celiac disease can lead to severe malnutrition, iron-deficiency anemia, osteoporosis, infertility, neurological complications, and a modestly increased risk of intestinal lymphoma. Early diagnosis and strict gluten-free diet adherence typically reverses intestinal damage and prevents these complications. Antibody levels normalize within months, and most patients achieve mucosal healing within 1–2 years.
Can Accurate Testing Prevent Unnecessary Dietary Restrictions?
Absolutely. Self-diagnosing gluten sensitivity without proper testing is common — and problematic. If someone goes gluten-free before celiac testing, blood tests and biopsies may produce false negatives, making diagnosis impossible without a gluten challenge. This means eating gluten for 6–8 weeks before retesting, which is difficult and uncomfortable. Proper testing first avoids this cycle entirely.
Does Proper Diagnosis Improve Nutritional Outcomes?
People with celiac disease need targeted monitoring for nutritional deficiencies, particularly iron, B12, folate, vitamin D, and calcium. Without a confirmed diagnosis, these deficiencies may go undetected. Additionally, a confirmed NCGS diagnosis may allow for a less restrictive gluten reduction (rather than strict avoidance), preserving access to nutrient-rich whole grains.
Does Distinguishing Between Conditions Guide Better Treatment?
Celiac disease requires lifelong, absolute gluten avoidance — even 20 ppm can trigger intestinal damage. NCGS management is more flexible. Some people with NCGS tolerate small amounts of gluten, sourdough bread, or ancient grains. The level of vigilance around cross-contamination differs dramatically between the two conditions.
What Are the Risks of Undiagnosed or Mismanaged Gluten-Related Disorders?
Untreated celiac disease carries significant health risks including malabsorption, bone loss, anemia, neurological damage, fertility problems, and increased cancer risk. Misdiagnosed NCGS may lead to unnecessary dietary restrictions that reduce nutritional intake, quality of life, and financial wellbeing.

Risks of untreated celiac disease include:
- Severe nutritional deficiencies — iron, B12, folate, fat-soluble vitamins (A, D, E, K), calcium, zinc, and magnesium
- Osteoporosis and fractures — due to calcium and vitamin D malabsorption
- Anemia — persistent iron-deficiency anemia unresponsive to supplementation
- Neurological complications — peripheral neuropathy, gluten ataxia, cognitive issues
- Reproductive problems — infertility, recurrent miscarriage, delayed puberty
- Secondary lactose intolerance — damaged villi can't produce lactase enzyme
- Associated autoimmune diseases — type 1 diabetes, autoimmune thyroid disease, Sjögren's syndrome
- Intestinal lymphoma — small but increased risk with prolonged untreated disease
- Dermatitis herpetiformis — intensely itchy blistering skin rash
For NCGS, the risks are primarily related to quality of life. Symptoms like chronic fatigue, brain fog, depression, and digestive discomfort can significantly impact daily functioning. However, there's no evidence of progressive intestinal damage or increased cancer risk.
How Should You Get Tested for Celiac Disease and Gluten Sensitivity?
The diagnostic pathway starts with celiac blood tests while you're still eating gluten, followed by endoscopic biopsy if blood tests are positive. NCGS is diagnosed by exclusion — after ruling out celiac disease and wheat allergy, an elimination diet followed by gluten reintroduction confirms the diagnosis.

Step 1: Serologic Blood Tests (While Eating Gluten)
The primary screening test is the tTG-IgA (tissue transglutaminase IgA antibody), which has 78–100% sensitivity and 90–100% specificity. Your doctor should also check total serum IgA to rule out IgA deficiency, which affects 2–3% of celiac patients and causes false negatives. For IgA-deficient patients, DGP-IgG (deamidated gliadin peptide IgG) is recommended.
:::warning[Safety Warning] You must be eating gluten daily (at least 1–2 servings) for 6–8 weeks before blood tests for accurate results. :::
Step 2: Endoscopy with Biopsy (Gold Standard for Celiac)
If serologic tests are positive, an upper endoscopy with duodenal biopsies confirms diagnosis. Updated 2026 European guidelines recommend at least four biopsy samples from the second part of the duodenum. Biopsies are graded using the Marsh classification, with Marsh Type 3 confirming symptomatic celiac disease.
Step 3: Genetic Testing (Optional)
HLA-DQ2/DQ8 genetic testing is useful for ruling out celiac disease. A negative result makes celiac disease extremely unlikely (99% negative predictive value). However, a positive result doesn't confirm celiac — it only indicates susceptibility.
Step 4: Diagnosing NCGS (By Exclusion)
After ruling out celiac disease and wheat allergy, remove gluten for 4–6 weeks. If symptoms improve, reintroduce gluten under medical supervision. If symptoms return, NCGS is the likely diagnosis. Consider that FODMAPs may be contributing to symptoms as well.
| Condition | Primary Tests | Key Notes |
|---|---|---|
| Celiac Disease | tTG-IgA + total IgA, then biopsy | Must be eating gluten for accurate results |
| Wheat Allergy | Skin prick test, wheat-specific IgE | Rapid onset symptoms (minutes to hours) |
| NCGS | Diagnosis of exclusion + elimination diet | No specific biomarkers available |
What Should You Eat and Avoid If You Have a Gluten-Related Disorder?
For celiac disease, a strict lifelong gluten-free diet is the only treatment — avoiding all wheat, barley, rye, and cross-contaminated foods. For NCGS, a gluten-reduced diet based on individual tolerance is typically sufficient, and some people may benefit more from a low-FODMAP approach than strict gluten avoidance.

Naturally Gluten-Free Foods
Focus on whole, naturally gluten-free foods: rice, quinoa, certified gluten-free oats, potatoes, corn, buckwheat, millet, amaranth, all fresh fruits and vegetables, legumes, nuts, seeds, meat, fish, eggs, and plain dairy. These provide essential nutrients that processed gluten-free products often lack.
Foods to Avoid (Celiac Disease — Strict Avoidance)
Eliminate all wheat (including spelt, farro, kamut, durum, semolina), barley, rye, triticale, malt, and brewer's yeast. Watch for hidden gluten in soy sauce, processed meats, salad dressings, medications, and supplements.
| Category | Contains Gluten | Gluten-Free Alternatives |
|---|---|---|
| Grains | Wheat, barley, rye, spelt, farro | Rice, quinoa, buckwheat, millet, amaranth |
| Pasta | Regular wheat pasta | Rice pasta, chickpea pasta, lentil pasta |
| Bread | Standard bread, rolls, wraps | Certified gluten-free bread, corn tortillas |
| Sauces | Soy sauce, some gravies | Tamari (gluten-free), coconut aminos |
| Beverages | Beer, malt beverages | Gluten-free beer, wine, cider, spirits |
Preventing Cross-Contamination (Critical for Celiac)
Use dedicated gluten-free toasters, cutting boards, and colanders. Avoid shared fryers, bulk bins, and contaminated condiment jars. Look for certified gluten-free products (under 20 ppm). When dining out, communicate your needs clearly and ask about preparation practices. Learn more about histamine and food reactions to manage multiple sensitivities.
Addressing Nutritional Gaps
Work with a registered dietitian to monitor and supplement common deficiencies. Prioritize iron-rich foods (leafy greens, legumes), calcium and vitamin D (dairy or fortified alternatives), B vitamins (meat, eggs, fortified gluten-free grains), and zinc (pumpkin seeds, shellfish). Regular blood work should track these levels, especially in the first year after diagnosis.
What Steps Should You Take First If You Suspect a Gluten-Related Disorder?
Start by continuing to eat gluten while seeking medical evaluation. The most critical mistake is going gluten-free before testing, which invalidates celiac blood tests and biopsies. Follow this phased approach for an accurate diagnosis and effective management plan.
Phase 1 — Get Tested (Weeks 1–2):
- Schedule appointment with gastroenterologist
- Continue eating gluten daily (do NOT go gluten-free yet)
- Request tTG-IgA + total serum IgA blood tests
- Keep a symptom journal documenting food intake and reactions
Phase 2 — Confirm Diagnosis (Weeks 2–6):
- If blood tests positive: schedule endoscopy with biopsy
- If celiac ruled out: get tested for wheat allergy (IgE testing)
- If both negative: discuss elimination diet with your doctor
Phase 3 — Implement Treatment (Weeks 6–12):
- Celiac confirmed: begin strict gluten-free diet with dietitian guidance
- NCGS confirmed: trial gluten reduction based on individual tolerance
- Get baseline nutritional blood work (iron, B12, folate, vitamin D, calcium, zinc)
- Start appropriate supplements for gut healing if deficient
Phase 4 — Long-Term Management (Ongoing):
- Annual follow-up with gastroenterologist (celiac)
- Repeat antibody testing to monitor adherence (celiac)
- Periodic nutritional blood work
- Connect with support groups (Celiac Disease Foundation, Beyond Celiac)

Top Recommended Products
Garden of
Garden of Life Vitamin Code Raw Iron
Celiac disease frequently causes iron-deficiency anemia due to malabsorption. This formula combines iron with vitamins C, B12, and folate — nutrients often depleted in celiac — plus probiotics for digestive comfort.
Pros
- + Gentle on stomach
- + includes B12 and folate for enhanced absorption
- + whole food sourced
- + gluten-free certified
Cons
- - Only 30-day supply per bottle
Why we included it: Celiac disease frequently causes iron-deficiency anemia due to malabsorption. This formula combines iron with vitamins C, B12, and folate — nutrients often depleted in celiac — plus probiotics for digestive comfort.
Retailer link opens on Amazon after the review details above
Thorne Zinc
Thorne Zinc Picolinate 30mg
Zinc deficiency is one of the most common nutritional gaps in celiac disease due to chronic diarrhea and malabsorption. Thorne's picolinate form provides superior absorption compared to other zinc forms.
Pros
- + Highly bioavailable picolinate form
- + NSF certified for purity
- + well-tolerated
- + gluten-free
Cons
- - May cause nausea if taken on empty stomach
Why we included it: Zinc deficiency is one of the most common nutritional gaps in celiac disease due to chronic diarrhea and malabsorption. Thorne's picolinate form provides superior absorption compared to other zinc forms.
Retailer link opens on Amazon after the review details above
NOW Foods
NOW Foods L-Glutamine Powder 1lb
L-glutamine is the primary energy source for enterocytes (intestinal lining cells) and plays a critical role in maintaining gut barrier integrity — especially important for people with celiac disease working to heal damaged intestinal tissue.
Pros
- + Primary fuel for intestinal cells
- + flexible dosing
- + unflavored and easy to mix
- + excellent value per serving
Cons
- - Large container
- - some may prefer capsule form
Why we included it: L-glutamine is the primary energy source for enterocytes (intestinal lining cells) and plays a critical role in maintaining gut barrier integrity — especially important for people with celiac disease working to heal damaged intestinal tissue.
Retailer link opens on Amazon after the review details above
Vital Proteins
Vital Proteins Collagen Peptides 20oz
Collagen provides the amino acids glycine, proline, and glutamine that support intestinal lining repair. For people with celiac disease working to heal damaged intestinal tissue, collagen supplementation offers broad connective tissue support.
Pros
- + Supports gut lining repair
- + also benefits skin
- + hair
- + and joints
- + dissolves easily in hot or cold liquids
- + neutral taste
Cons
- - Bovine-sourced (not suitable for vegetarians)
- - premium price point
Why we included it: Collagen provides the amino acids glycine, proline, and glutamine that support intestinal lining repair. For people with celiac disease working to heal damaged intestinal tissue, collagen supplementation offers broad connective tissue support.
Retailer link opens on Amazon after the review details above
Further Reading
Further Reading
"Celiac Disease: A Hidden Epidemic"
by Peter H.R. Green, MD, and Rory Jones
Comprehensive medical overview of celiac disease; diagnostic guidance; practical dietary advice; recipes and meal planning strategies
Why it adds value here
Dr. Green is one of the world's foremost celiac disease researchers. This book translates decades of clinical expertise into accessible guidance that empowers patients to manage their condition confidently.
Best for: Anyone newly diagnosed with celiac disease or suspecting gluten-related issues
View book detailsFurther Reading
"Gluten Freedom"
by Alessio Fasano, MD, and Susie Flaherty
Cutting-edge research on celiac disease, NCGS, and wheat allergy; diagnostic frameworks; dietary management; latest scientific discoveries on intestinal permeability
Why it adds value here
Dr. Fasano is a pioneer in celiac and gluten sensitivity research whose work on zonulin and intestinal permeability has shaped modern understanding of gluten-related disorders.
Best for: People seeking a deep scientific understanding of all gluten-related disorders
View book detailsAEO FAQ
Frequently Asked Questions
12 common questions answered
Celiac disease is an autoimmune disorder where gluten triggers intestinal damage (villous atrophy), while non-celiac gluten sensitivity causes symptoms without autoimmune activity or intestinal damage. Celiac disease is diagnosed through blood antibodies and biopsy, whereas NCGS is a diagnosis of exclusion after ruling out celiac and wheat allergy.
Yes, celiac disease can develop at any age. While many people are diagnosed in childhood, a significant number develop symptoms in their 40s, 50s, or even later. Triggers may include stress, pregnancy, surgery, or viral infections in genetically susceptible individuals.
No — this is the most important rule in celiac testing. You must be eating gluten regularly (at least 1–2 servings daily for 6–8 weeks) for blood tests and biopsies to be accurate. Going gluten-free before testing causes false negative results.
Current research suggests NCGS does not progress to celiac disease. They are considered separate conditions with different immune mechanisms. However, if you have NCGS, periodic retesting for celiac disease may be recommended, as initial testing can sometimes produce false negatives.
None. Even trace amounts below 20 parts per million (ppm) can trigger intestinal damage in celiac disease. This is why strict avoidance and cross-contamination prevention are essential. The FDA defines "gluten-free" as containing less than 20 ppm.
No. Wheat allergy is an IgE-mediated allergic reaction to wheat proteins that can cause hives, swelling, and anaphylaxis within minutes. Celiac disease is an autoimmune condition with delayed intestinal damage. People with wheat allergy may tolerate barley and rye, while people with celiac cannot.
Iron, vitamin B12, folate, calcium, vitamin D, and zinc are the most common deficiencies. These result from malabsorption caused by damaged intestinal villi. Supplementation and regular blood monitoring are recommended, especially in the first year after diagnosis.
Most people with celiac disease can safely eat certified gluten-free oats. Pure oats are naturally gluten-free, but conventional oats are frequently cross-contaminated with wheat during growing and processing. Always choose oats specifically labeled "certified gluten-free."
Symptoms typically improve within 2–4 weeks of starting a strict gluten-free diet. Antibody levels may take several months to normalize. Full intestinal healing (mucosal recovery) usually takes 1–2 years in adults, though some individuals may take longer.
NCGS is recognized as a real clinical entity by major gastroenterology organizations. However, a 2026 Lancet review found that only 16–30% of self-reported cases had symptoms specifically triggered by gluten in controlled studies. FODMAPs, ATIs, and nocebo effects contribute to symptoms in many cases.
Testing is recommended for anyone with chronic digestive symptoms, unexplained iron-deficiency anemia, unexplained osteoporosis, type 1 diabetes, autoimmune thyroid disease, dermatitis herpetiformis, or a first-degree relative with celiac disease. First-degree relatives have approximately a 10% risk.
Not necessarily. Many processed gluten-free products are lower in fiber, B vitamins, and iron compared to their gluten-containing counterparts, and may be higher in sugar, fat, and sodium. The healthiest gluten-free diet emphasizes naturally gluten-free whole foods rather than processed substitutes.
Was this article helpful?
Written & Reviewed By Experts
Author
Dr. Lisa Nakamura
Medical Reviewer
Dr. Sarah Chen
All content is evidence-based, peer-reviewed by qualified professionals, and updated regularly. Our editorial team follows strict guidelines for accuracy and transparency.
References & Citations
18 sources cited
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Read the full medical disclaimer. Always consult with a qualified healthcare provider before starting any new supplement, treatment, or major dietary change.