Heavy metals are everywhere — in contaminated water, old paint, dental fillings, certain foods, and industrial pollutants. Over time, chronic low-level exposure to lead, mercury, arsenic, and cadmium can accumulate in tissues and contribute to neurological damage, cardiovascular disease, kidney dysfunction, and even cancer [1]. A 2024 review confirmed that aluminum, cadmium, arsenic, mercury, and lead play significant roles in gastrointestinal, pulmonary, kidney, reproductive, neurodegenerative, and cardiovascular diseases [2].
The good news? Your body already has detoxification pathways designed to handle toxic metals — but they can become overwhelmed. This evidence-based guide walks you through safe chelation strategies, from getting properly tested to supporting your body's natural detox systems and knowing when medical intervention is warranted.
What Do You Need to Know Before Starting a Heavy Metal Detox?
Before beginning any heavy metal detox protocol, you need a confirmed diagnosis through validated testing, a clear understanding of your exposure sources, and a plan that matches the severity of your burden. Attempting aggressive chelation without proper preparation can redistribute metals to more sensitive tissues, potentially causing more harm than the original exposure.
Heavy metal detoxification is not a one-size-fits-all process. The approach for someone with confirmed lead poisoning from occupational exposure is fundamentally different from someone with low-level accumulated burden from environmental sources. Here's what to consider:
Who should consider heavy metal detox:
- People with confirmed elevated heavy metal levels on validated testing
- Those with known occupational exposure (mining, battery manufacturing, painting, welding)
- Individuals with chronic symptoms consistent with heavy metal toxicity (fatigue, brain fog, neuropathy, GI issues)
- Those living in older homes with lead paint or lead pipes
Expected timeline:
- Mild burden with natural support: 3–6 months
- Moderate burden with medical chelation: 6–12 months with multiple rounds
- Severe poisoning: Ongoing medical management
Prerequisites:
- Adequate kidney and liver function (chelation stresses both organs)
- Sufficient mineral status (zinc, selenium, magnesium) — chelators can deplete essential minerals
- Healthy gut function for proper excretion
Step 1: How Do You Get Properly Tested for Heavy Metals?
The gold standard for heavy metal testing uses blood tests for lead and organic mercury, and urine tests for arsenic and cadmium. These validated methods provide reliable baselines — blood lead levels above 5 µg/dL in adults are considered elevated by the CDC, while mercury levels above 5.8 µg/L warrant further evaluation.
Which tests should you request from your doctor?
Start with these evidence-based tests depending on your suspected exposure:
- Lead: Whole blood lead level (venous draw, not fingerstick). Reference: <5 µg/dL (CDC updated threshold). Levels >25 µg/dL may require chelation [3].
- Mercury: Whole blood mercury for organic/methylmercury exposure (primarily from fish). Reference: <5.8 µg/L. For inorganic mercury (dental amalgams, occupational), urine mercury is more appropriate.
- Arsenic: 24-hour urine collection or spot urine. Avoid seafood for 48 hours before testing (organic arsenic from seafood can cause false elevations).
- Cadmium: Urine cadmium reflects chronic exposure. Blood cadmium reflects recent exposure. Reference: urine <1 µg/L.
What about provoked urine testing?
Provoked urine testing (also called "challenge testing") involves taking a chelating agent and then measuring metal excretion in urine. While some integrative practitioners use this method, it remains controversial. A 2021 study found that provoked urine testing had a positive predictive value of only 4.3% for diagnosing heavy metal poisoning — meaning over 95% of "positive" results were false positives [4]. The American College of Medical Toxicology (ACMT) advises against its use for diagnosis [5].
Step 2: How Do You Identify and Remove Ongoing Exposure Sources?
Removing ongoing heavy metal exposure is the most critical step in any detox protocol — without it, chelation simply creates a revolving door where metals are removed and reabsorbed simultaneously. Identify your primary exposure sources through testing results, occupational history, home environment assessment, and dietary analysis.
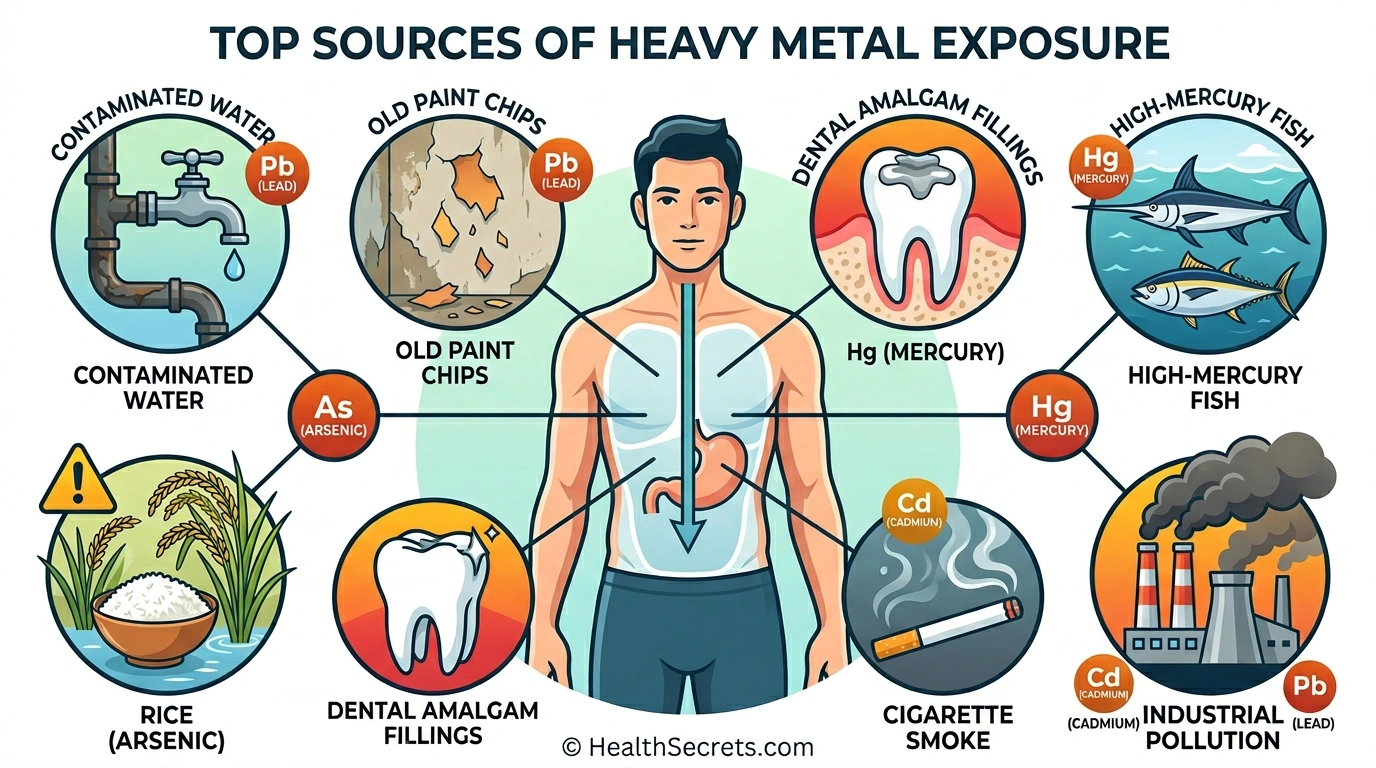
Common exposure sources by metal:
Lead:
- Homes built before 1978 (lead paint)
- Old plumbing with lead pipes or lead solder
- Some imported ceramics, toys, and cosmetics
- Occupational: construction, battery recycling, shooting ranges
Mercury:
- High-mercury fish: shark, swordfish, king mackerel, tilefish, bigeye tuna
- Dental amalgam fillings (consult a biological dentist for safe removal — improper removal can spike mercury levels)
- Some skin-lightening creams
- Broken CFL bulbs or old thermometers
Arsenic:
- Well water in certain geographic areas
- Rice and rice products (rice accumulates arsenic from soil)
- Pressure-treated wood (CCA-treated, pre-2004)
Cadmium:
- Cigarette smoke (primary source for most people)
- Contaminated soil (near industrial areas)
- Some shellfish and organ meats
Action steps:
- Test your home water supply (use an NSF-certified lab)
- If you have young children, test for lead paint in pre-1978 homes
- Limit high-mercury fish to 1–2 servings per week; choose low-mercury options (salmon, sardines, anchovies)
- Rinse rice thoroughly and cook in excess water (reduces arsenic by 40–60%)
- If you smoke, quitting is the single most effective way to reduce cadmium exposure
Step 3: How Do You Support Your Body's Natural Detox Pathways?
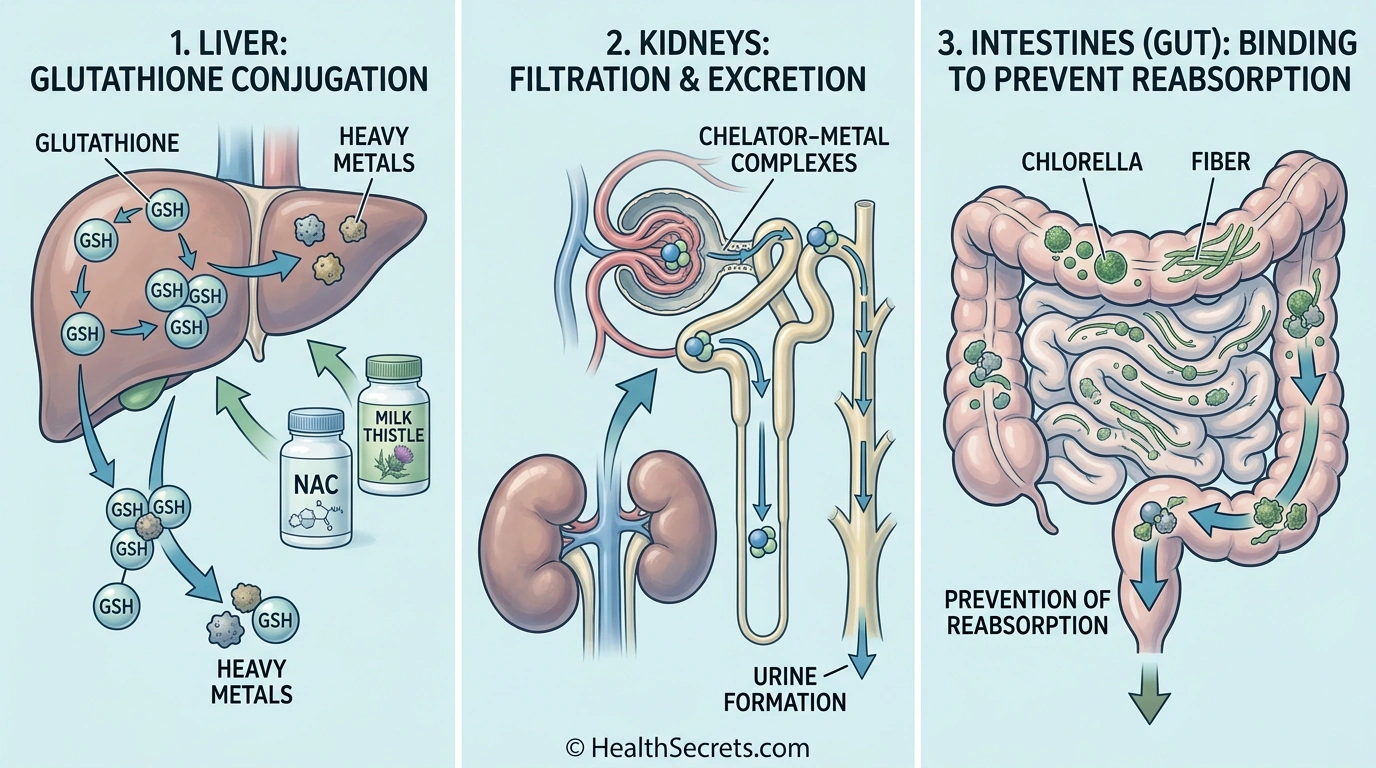
Your liver, kidneys, and gut are the three primary exit routes for heavy metals, and optimizing their function creates the foundation for effective detoxification. Support these pathways with targeted nutrients — NAC (600–1,200 mg/day) boosts glutathione production, milk thistle (150–300 mg silymarin) protects liver cells, and adequate fiber (30+ g/day) prevents reabsorption through the gut.
How does glutathione help remove heavy metals?
Glutathione is your body's master detoxification molecule and plays a central role in heavy metal excretion. It directly binds to mercury, lead, arsenic, and cadmium, forming conjugates that are excreted through bile and urine. NAC (N-acetyl cysteine) is the most effective way to raise glutathione levels, as it provides the rate-limiting amino acid cysteine [6]. For direct supplementation, liposomal glutathione offers superior absorption compared to standard forms.
Learn more about glutathione's role in detox: Glutathione: The Master Antioxidant for Detox and Cellular Health
Which supplements support liver detox pathways?
- NAC (N-Acetyl Cysteine): 600–1,200 mg/day. Precursor to glutathione. Supports Phase II liver detox. Well-studied for heavy metal protection [6].
- Milk Thistle (Silymarin): 150–300 mg/day standardized to 80% silymarin.
Hepatoprotective — shields liver cells during chelation. Has demonstrated protective effects against lead and mercury-induced liver damage in animal studies [7].
- Alpha-Lipoic Acid (ALA): 300–600 mg/day. Chelates mercury and arsenic. Crosses blood-brain barrier (unique among natural chelators). Use with caution — can redistribute mercury if dental amalgams are still present.
- Selenium: 200 mcg/day. Binds mercury to form inert selenium-mercury complexes. Protective against mercury toxicity [8].
For comprehensive liver support strategies: How to Detox Your Liver Naturally
How does gut health affect heavy metal excretion?
Your gut is the final checkpoint for metal excretion. Metals conjugated by the liver are excreted into bile, enter the intestines, and must be eliminated before they can be reabsorbed (enterohepatic recirculation). Supporting this process requires:
- Fiber: 30+ g/day from vegetables, flaxseed, and psyllium binds metals in the gut
- Chlorella: Binds metals in the GI tract, potentially preventing reabsorption. A human study showed mercury and tin reduction after 90 days of algae supplementation [9], and animal studies demonstrate lead-binding capacity [10]
- Activated charcoal: Can bind metals in the gut when taken away from meals and supplements (2+ hours apart)
- Probiotics: Support gut barrier integrity and may reduce metal absorption
For a complete gut detox protocol: Gut Detox Protocol: Restore Your Digestive Health
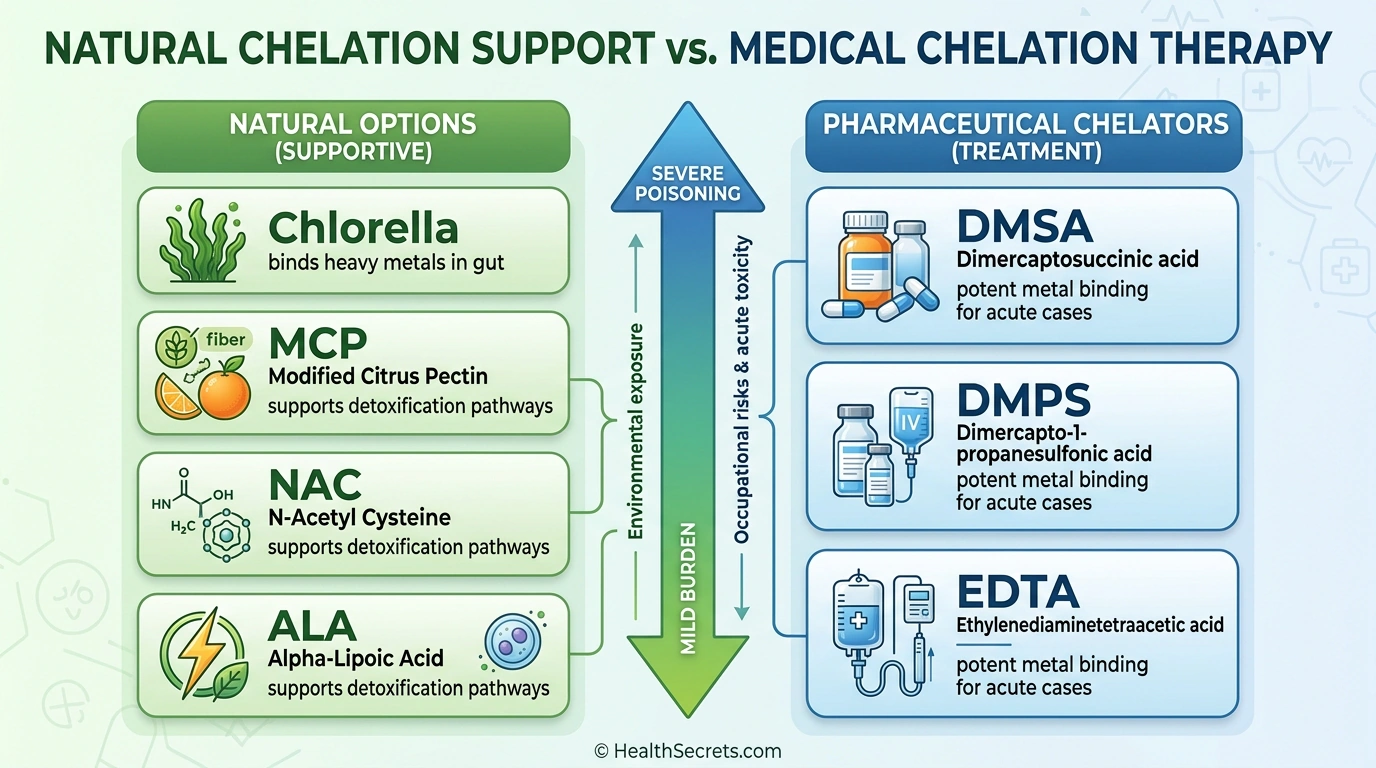
Step 4: How Do You Use Natural Chelation Support Safely?
Natural chelation agents like modified citrus pectin, chlorella, and cilantro extract can gently mobilize and bind low-level heavy metal burdens without the aggressive action of pharmaceutical chelators. Modified citrus pectin showed a 74% average decrease in toxic heavy metals across five case studies, while chlorella demonstrated mercury reduction in a 90-day human trial [9][11].
What is modified citrus pectin and how does it chelate metals?
Modified citrus pectin (MCP) is a specially processed form of citrus pectin with smaller molecular weight that allows it to enter the bloodstream. Unlike regular pectin (which only works in the gut), MCP can chelate metals systemically. In a pilot study of five participants, MCP supplementation (15 g/day) produced a 74% average decrease in toxic heavy metals (lead, mercury, cadmium, arsenic) measured in urine excretion [11]. A separate study in children found that MCP significantly increased urinary lead excretion without depleting essential minerals [12].
Dosing: 5–15 g/day, mixed in water, taken between meals.
How effective is chlorella for heavy metal binding?
Chlorella (Chlorella vulgaris) has a unique cell wall structure that binds heavy metals in the gastrointestinal tract. While most robust evidence comes from animal studies — including a recent study showing significant lead removal in rats [10] — a human clinical study found that 90 days of chlorella combined with Fucus algae significantly reduced blood mercury and tin levels [9]. Chlorella works best as an ongoing binder during active chelation to prevent gut reabsorption.
Dosing: 3–6 g/day (tablets or powder), with meals.
What role does activated charcoal play in metal detox?
Activated charcoal binds a wide range of toxins including some heavy metals in the GI tract. It is most useful as an adjunct during active detox protocols to prevent reabsorption. However, it also binds medications and supplements, so timing is critical.
Dosing: 560–1,120 mg, taken 2+ hours away from food, supplements, and medications.
For more on activated charcoal protocols: Activated Charcoal: The Complete Detox Guide
NOW Foods NAC 600mg
Editor's ChoiceNOW Foods · Foundation of any heavy metal detox protocol — boosts glutathione, the body's master detox molecule
NOW Foods Chlorella 1000mg
Best for GI BindingNOW Foods · Binding heavy metals in the gut to prevent reabsorption during chelation protocols
EcoNugenics PectaSol-C Modified Citrus Pectin
Best for Systemic ChelationEcoNugenics PectaSol-C · Gentle systemic heavy metal removal without depleting essential minerals
Jarrow Formulas Milk Thistle 150mg
Best for Liver ProtectionJarrow Formulas · Protecting liver cells during active chelation and detox protocols
Quicksilver Scientific Liposomal Glutathione
Best for Direct GlutathioneQuicksilver Scientific · Rapidly raising glutathione levels when NAC alone isn't sufficient
NOW Foods Selenium 200mcg
Best for Mercury ProtectionNOW Foods · Forming protective selenium-mercury complexes that reduce mercury toxicity
Nature's Way Activated Charcoal 560mg
Best for Acute BindingNature's Way · Emergency GI-level binding of heavy metals and toxins during active chelation rounds
Read the detailed review cards below before opening any retailer link
Top Recommended Products

NOW Foods
NOW Foods NAC 600mg
NAC is the most well-researched supplement for raising glutathione levels, which is essential for binding and excreting heavy metals through Phase II liver detoxification.
Pros
- + Clinically validated glutathione precursor
- + excellent value per dose
- + well-tolerated at therapeutic doses
Cons
- - May cause GI upset in sensitive individuals
- - sulfur smell
- - high doses may thin mucus excessively
Why we included it: NAC is the most well-researched supplement for raising glutathione levels, which is essential for binding and excreting heavy metals through Phase II liver detoxification.
Retailer link opens on Amazon after the review details above

NOW Foods
NOW Foods Chlorella 1000mg
Chlorella's unique cell wall structure physically binds mercury, lead, and cadmium in the GI tract, and a 90-day human study confirmed significant mercury and tin reduction.
Pros
- + Human studies support mercury reduction
- + broken cell wall improves nutrient absorption
- + doubles as a nutrient-dense green superfood
Cons
- - Earthy taste may bother some
- - tablets are large
- - primarily GI-level action (doesn't chelate systemically)
Why we included it: Chlorella's unique cell wall structure physically binds mercury, lead, and cadmium in the GI tract, and a 90-day human study confirmed significant mercury and tin reduction.
Retailer link opens on Amazon after the review details above

EcoNugenics PectaSol-C
EcoNugenics PectaSol-C Modified Citrus Pectin
PectaSol is the only modified citrus pectin with published clinical evidence for heavy metal reduction, and uniquely works systemically rather than only in the GI tract.
Pros
- + Clinical evidence showing 74% average decrease in toxic metals
- + does not deplete essential minerals
- + gentle enough for long-term use
Cons
- - Premium price
- - powder requires mixing
- - large daily dose (up to 15 g)
Why we included it: PectaSol is the only modified citrus pectin with published clinical evidence for heavy metal reduction, and uniquely works systemically rather than only in the GI tract.
Retailer link opens on Amazon after the review details above

Jarrow Formulas
Jarrow Formulas Milk Thistle 150mg
Chelation stresses the liver significantly, and milk thistle's silymarin has demonstrated protective effects against lead and mercury-induced liver damage in multiple studies.
Pros
- + Gold-standard silymarin standardization
- + exceptional value for 200 capsules
- + well-researched hepatoprotective effects
Cons
- - Benefits are primarily protective (won't chelate metals directly)
- - may interact with certain medications metabolized by the liver
Why we included it: Chelation stresses the liver significantly, and milk thistle's silymarin has demonstrated protective effects against lead and mercury-induced liver damage in multiple studies.
Retailer link opens on Amazon after the review details above

Quicksilver Scientific
Quicksilver Scientific Liposomal Glutathione
When you need to raise glutathione levels quickly — especially at the start of a heavy metal protocol — liposomal delivery bypasses the digestive breakdown that renders standard glutathione supplements largely ineffective.
Pros
- + Highest bioavailability glutathione form available
- + liposomal technology preserves active molecule
- + fast-acting
Cons
- - Premium price
- - requires refrigeration after opening
- - taste may be unpleasant
Why we included it: When you need to raise glutathione levels quickly — especially at the start of a heavy metal protocol — liposomal delivery bypasses the digestive breakdown that renders standard glutathione supplements largely ineffective.
Retailer link opens on Amazon after the review details above

NOW Foods
NOW Foods Selenium 200mcg
Selenium forms inert selenium-mercury complexes in the body, directly reducing mercury's toxic effects, making it essential for anyone with mercury exposure.
Pros
- + Essential mineral with direct mercury-binding properties
- + affordable
- + supports thyroid function and antioxidant defense simultaneously
Cons
- - Upper limit is 400 mcg/day (toxicity possible at higher doses)
- - may interact with certain medications
- - Brazil nuts provide a food alternative
Why we included it: Selenium forms inert selenium-mercury complexes in the body, directly reducing mercury's toxic effects, making it essential for anyone with mercury exposure.
Retailer link opens on Amazon after the review details above

Nature's Way
Nature's Way Activated Charcoal 560mg
Activated charcoal is a useful adjunct during active chelation rounds to bind mobilized metals in the gut and prevent enterohepatic recirculation.
Pros
- + Broad-spectrum toxin binder
- + well-established safety profile
- + affordable
Cons
- - Must be taken well away from food and other supplements (binds them too)
- - may cause constipation
- - not specific to heavy metals
Why we included it: Activated charcoal is a useful adjunct during active chelation rounds to bind mobilized metals in the gut and prevent enterohepatic recirculation.
Retailer link opens on Amazon after the review details above
Step 5: When Should You Consider Medical Chelation Therapy?
Medical chelation therapy is warranted when blood lead levels exceed 25 µg/dL in adults (or 45 µg/dL in children), when mercury levels remain persistently elevated despite source removal, or when you have documented symptoms of acute heavy metal poisoning. Always pursue medical chelation under the direct supervision of a toxicologist or experienced physician — never self-administer pharmaceutical chelators.
What are the FDA-approved chelation agents?
- DMSA (Succimer/Chemet): FDA-approved for lead poisoning in children. Oral administration makes it the most accessible chelator. A case series of 17 lead-poisoned adults showed DMSA increased lead excretion by a factor of 12 [13]. Also effective for mercury and arsenic.
- DMPS (Unithiol): Not FDA-approved in the US but widely used in Europe. Particularly effective for mercury chelation. Available through compounding pharmacies [13].
- CaNa₂EDTA (Calcium Disodium EDTA): IV administration. Used for severe lead poisoning. The TACT trial demonstrated an 18% relative risk reduction in cardiovascular events in post-MI patients [14]. However, the 2024 TACT2 trial found that while EDTA reduced blood lead by 60%, it showed no significant cardiovascular benefit in diabetic post-MI patients [15].
- D-Penicillamine: Oral chelator for copper (Wilson's disease) and sometimes lead. More side effects than DMSA.
What does a typical medical chelation protocol look like?
Medical chelation follows a cycle-and-rest pattern:
- Chelation round: 3–5 days of chelator administration (oral DMSA or IV EDTA)
- Rest period: 7–14 days off to allow kidney recovery and mineral replenishment
- Mineral supplementation: Zinc, selenium, magnesium between rounds (chelators deplete essential minerals)
- Monitoring: Blood/urine metals and kidney function before each round
- Repeat: Multiple rounds until levels normalize (typically 5–20+ rounds depending on burden)
:::warning[Critical warning] The FDA has not approved any OTC chelation products including supplements marketed as chelators, nasal sprays, suppositories, or clay baths [16]. These unregulated products can be dangerous. :::
Step 6: How Do You Monitor Progress and Know When You're Done?
Monitor your heavy metal detox progress by retesting blood and urine levels every 3–6 months using the same laboratory and collection method as your baseline. Successful detox shows a consistent downward trend in metal levels combined with symptom improvement — a single test is never sufficient to declare completion.
What markers should you track?
- Primary metals: Retest the same metals from your baseline (lead, mercury, arsenic, cadmium)
- Kidney function: BUN, creatinine, GFR — chelation stresses the kidneys
- Liver enzymes: ALT, AST — monitor liver health during the protocol
- Essential minerals: Zinc, selenium, magnesium, copper, iron — chelation can deplete these
- Symptoms journal: Track energy, cognition, GI function, neuropathy, sleep quality monthly
When can you stop the protocol?
Consider your detox protocol complete when:
- Metal levels are within reference ranges on two consecutive tests (3 months apart)
- Symptoms have meaningfully improved or resolved
- Essential mineral levels remain stable
- Your healthcare provider confirms it's safe to discontinue
After completing active detox, transition to a maintenance phase: continue NAC (600 mg/day), eat a mineral-rich diet, maintain gut health, limit ongoing exposures, and retest annually.
What Are the Most Common Heavy Metal Detox Mistakes to Avoid?
The most dangerous mistake is attempting aggressive chelation without proper testing or medical supervision — this can redistribute metals from tissues to the brain, kidneys, or other sensitive organs. Other common errors include chelating while dental amalgams are still present, neglecting mineral replacement, and expecting overnight results from a process that takes months.
Top mistakes and how to avoid them:
- Chelating without testing first. You need a baseline to know what you're dealing with and to measure progress. Random supplement protocols based on symptoms alone are inefficient at best and dangerous at worst.
- Ignoring ongoing exposure. Chelation while you're still being exposed is like bailing water from a sinking boat without plugging the hole. Address sources first.
- Using alpha-lipoic acid with amalgam fillings. ALA crosses the blood-brain barrier and can redistribute mercury from fillings directly into brain tissue. Remove amalgams first (by a qualified biological dentist), wait 3 months, then consider ALA.
- Neglecting mineral replacement. All chelators — natural and pharmaceutical — bind some essential minerals along with toxic metals. Supplement zinc (30 mg), selenium (200 mcg), and magnesium (400 mg) between chelation rounds.
- Expecting fast results. Heavy metals accumulate in bones and deep tissues over decades. Safe removal takes months to years. Aggressive protocols that promise rapid detox often cause redistribution injuries.
- Ignoring gut health. If your gut is compromised (constipation, leaky gut, dysbiosis), mobilized metals can be reabsorbed instead of excreted. Fix gut function before intensive chelation.
- Falling for unproven products. Detox foot pads, ionic foot baths, zeolite sprays, and infrared sauna "metal detox" have no reliable evidence for heavy metal removal. Stick to evidence-based approaches.
For a comprehensive foundation: The Complete Guide to Detox and Cleansing
Is Heavy Metal Chelation Safe? When Should You Stop?
Heavy metal chelation is generally safe when performed under medical supervision with proper monitoring, but all chelation carries risks including mineral depletion, kidney stress, and potential metal redistribution. Stop immediately and contact your doctor if you experience worsening symptoms, signs of kidney problems (reduced urination, swelling), severe GI distress, or neurological changes.
What are the main risks of chelation?
- Mineral depletion: Chelators bind essential minerals (zinc, copper, iron, calcium). Without replacement, this can cause deficiencies with serious consequences.
- Kidney stress: Metals bound to chelators are excreted through the kidneys. Pre-existing kidney disease increases risk.
- Metal redistribution: Improper chelation can move metals from less harmful storage sites (bone, fat) to more sensitive organs (brain, kidneys).
- Herxheimer-like reactions: Mobilizing stored metals can temporarily worsen symptoms — fatigue, headaches, GI upset. Mild reactions are expected; severe reactions mean the protocol is too aggressive.
Who should NOT attempt chelation?
- People with kidney disease or impaired kidney function
- Pregnant or breastfeeding women (mobilized metals can cross the placenta and enter breast milk)
- People with severe liver disease
- Anyone taking medications with known chelator interactions (consult your pharmacist)
- Children (must be under pediatric toxicology supervision)
What Should You Do First to Start a Safe Heavy Metal Detox?
Start with validated testing to establish your baseline, then systematically remove exposure sources before adding any chelation support. This phased approach prevents the common mistake of chelating metals that are still actively entering your body, which reduces effectiveness and increases side effects.
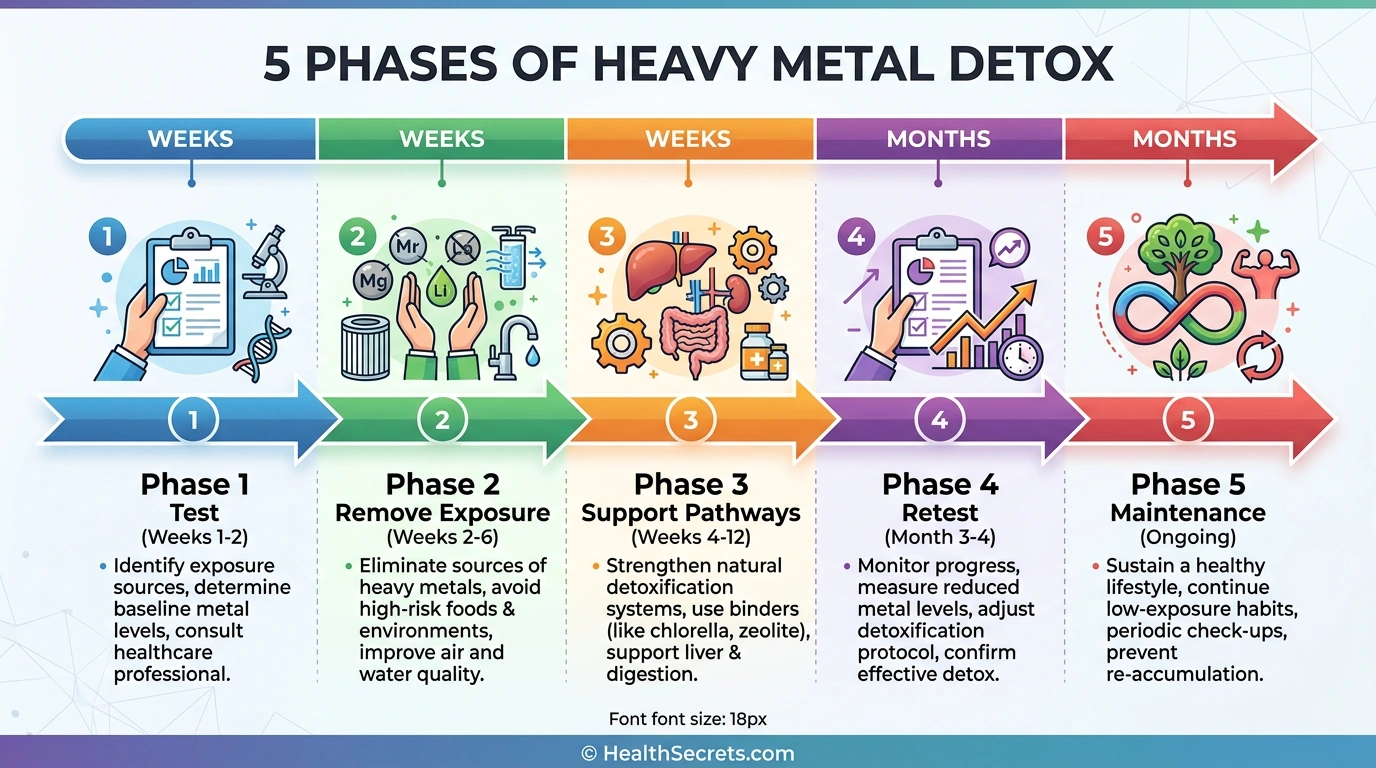
Phase 1 — Test and Assess (Weeks 1–2):
- Request blood lead and blood mercury tests from your doctor
- Request 24-hour urine arsenic and cadmium tests
- Complete an exposure assessment (home, work, diet, dental history)
- Test your home water supply for heavy metals
- Get baseline kidney function (BUN, creatinine) and liver enzymes (ALT, AST)
Phase 2 — Remove Exposure (Weeks 2–6):
- Address identified exposure sources (water filter, diet changes, occupational protection)
- Switch to low-mercury fish (salmon, sardines, anchovies)
- If dental amalgams are a concern, consult a biological dentist for evaluation
- Begin mineral optimization: zinc 30 mg, selenium 200 mcg, magnesium 400 mg daily
Phase 3 — Support Detox Pathways (Weeks 4–12):
- Start NAC 600 mg twice daily to boost glutathione
- Add milk thistle 150 mg (standardized to 80% silymarin) twice daily
- Increase dietary fiber to 30+ g/day
- Add chlorella 3 g/day with meals as a gut binder
- Consider modified citrus pectin 5–15 g/day between meals
Phase 4 — Retest and Evaluate (Month 3–4):
- Retest all baseline metals using the same lab and method
- Review symptom journal for improvements
- If levels remain significantly elevated, consult a toxicologist about medical chelation
- If levels are trending down, continue natural support for another 3 months
Phase 5 — Maintenance (Ongoing):
- Continue NAC 600 mg/day and mineral supplementation
- Maintain clean diet with adequate fiber
- Retest annually or as recommended by your doctor
- Stay vigilant about new exposure sources