Here's something most people don't realize: inflammation can simmer beneath the surface for years — quietly damaging your blood vessels, joints, and organs — without you feeling a thing. No fever. No swelling. Just a slow, silent process that increases your risk of heart disease, diabetes, and even cancer.
The good news? A simple blood test can reveal what's happening inside.
Inflammation markers are proteins and other substances in your blood that rise when your body is fighting something — whether it's an infection, an autoimmune flare, or the kind of low-grade chronic inflammation that drives most modern diseases. Understanding these markers gives you (and your doctor) a window into what's really going on.
But here's the tricky part: elevated markers don't tell you why inflammation is happening. They're like a smoke alarm — they alert you to a problem, but you still need to find the fire. And different markers behave differently. CRP shoots up within hours of an injury. ESR takes its time. Ferritin plays double duty as both an iron storage protein and an inflammation signal.
In this guide, you'll learn exactly what each inflammation marker measures, what the numbers actually mean, when testing makes sense, and — most importantly — what you can do if your levels come back high.
If you're new to the topic of inflammation, start with our complete guide to chronic inflammation for the foundational science. For dietary strategies, check out our anti-inflammatory diet guide.
What Are Inflammation Markers and Why Should You Care?
Inflammation markers are proteins and other substances in your blood that increase in response to inflammation anywhere in the body. They act as measurable signals — produced mainly by the liver — that help clinicians detect, diagnose, and monitor inflammatory conditions ranging from acute infections to chronic diseases like cardiovascular disease and autoimmune disorders.
The concept is straightforward. When your body encounters a threat — a bacterial infection, tissue damage, or even persistent metabolic stress from obesity — your immune system launches an inflammatory response. As part of that response, the liver ramps up production of specific proteins called acute phase reactants. These proteins circulate in your blood and can be measured with standard laboratory tests.
There are two broad categories to understand:
What Is Acute Inflammation and How Does It Show Up in Blood Tests?
Acute inflammation is your body's rapid, short-term response to injury or infection. It's the redness, swelling, and heat you feel around a cut or sprained ankle. In blood tests, acute inflammation causes a sharp, dramatic spike in markers like CRP — often rising 100-fold or more within 24–48 hours. This kind of elevation typically resolves once the underlying issue is treated.
What Is Chronic Inflammation and Why Is It Harder to Detect?
Chronic inflammation is a persistent, low-grade process that can continue for months or years without obvious symptoms. It's linked to conditions like heart disease, type 2 diabetes, Alzheimer's, and cancer. Blood markers may be only mildly elevated — which is why high-sensitivity tests like hs-CRP were developed. Detecting this kind of inflammation early gives you a chance to intervene before serious damage occurs.
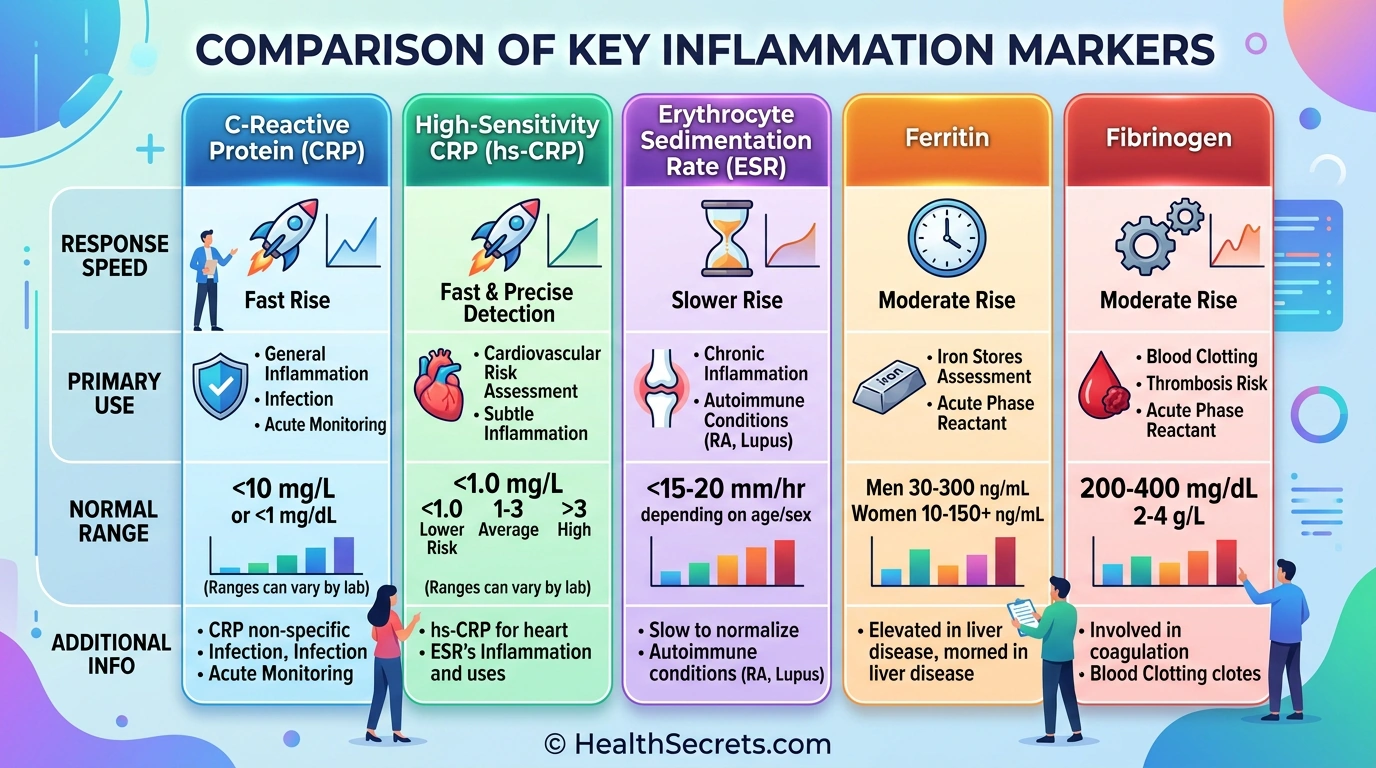
The most commonly ordered inflammation markers in clinical practice include:
| Marker | What It Measures | Speed of Response | Primary Clinical Use |
|---|---|---|---|
| CRP | Acute phase protein from liver | Rises within 6 hours | Infection, acute inflammation |
| hs-CRP | Same protein, higher sensitivity | Detects low-grade levels | Cardiovascular risk assessment |
| ESR | Red blood cell settling rate | Rises over hours to days | Autoimmune disease monitoring |
| Ferritin | Iron storage + acute phase reactant | Variable | Iron status and inflammation |
| Fibrinogen | Clotting protein + acute phase reactant | Rises within 24–48 hours | CVD risk, clotting risk |
How Do Inflammation Markers Work in the Body?
Inflammation markers work through a cascade that begins with your immune system detecting a threat and ends with your liver producing measurable proteins. Understanding this process helps you make sense of why certain markers rise faster than others — and why no single marker can tell you everything.
When tissue damage or infection occurs, immune cells at the site release signaling molecules called cytokines — primarily interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-alpha). These cytokines travel through the bloodstream to the liver, where they trigger the production of acute phase reactants like CRP and fibrinogen.
How Does CRP Respond to Inflammation?
CRP is the fastest and most sensitive general inflammation marker available in routine clinical testing. When IL-6 signals the liver, CRP production begins within hours. Levels can rise from a normal baseline of less than 1 mg/L to over 100 mg/L within 24–48 hours during a serious infection. CRP has a short half-life of about 19 hours, which means it drops quickly once the inflammatory stimulus is removed — making it useful for monitoring treatment response in real time. [2]

How Is ESR Different from CRP?
ESR doesn't measure a specific protein. Instead, it measures how quickly red blood cells settle to the bottom of a test tube over one hour (reported in mm/hr). During inflammation, the liver produces more fibrinogen and immunoglobulins, which cause red blood cells to clump together and settle faster. Because ESR depends on these larger proteins accumulating, it responds more slowly than CRP — rising over days rather than hours. ESR is also influenced by non-inflammatory factors like anemia, age, and gender, which makes it less specific but still valuable for tracking chronic conditions. [4]
What Role Does Ferritin Play as an Inflammation Marker?
Ferritin complicates things because it wears two hats. Primarily, it's your body's main iron storage protein — low ferritin means low iron stores. But ferritin is also an acute phase reactant that rises during inflammation regardless of iron status. This dual role means an "normal" or "high" ferritin level in someone with active inflammation could actually be masking iron deficiency. Clinicians need to interpret ferritin alongside CRP or other markers to distinguish between true iron sufficiency and inflammation-driven elevation. [11]
How Do Cytokines Like IL-6 and TNF-Alpha Fit In?
IL-6 and TNF-alpha are the upstream signaling molecules that cause markers like CRP to rise. They're measured primarily in research settings because the tests are expensive, require specialized labs, and aren't part of routine clinical practice. However, understanding their role helps explain why inflammation markers behave the way they do — IL-6 directly stimulates CRP production, which is why CRP tracks so closely with the inflammatory response.
What Are the Key Benefits of Inflammation Testing?
Inflammation marker testing provides clinicians with objective, measurable data about what's happening inside your body — information that symptoms alone can't always reveal. Used correctly, these tests can detect hidden inflammation, guide treatment decisions, predict disease risk, and track whether interventions are actually working.
Can Inflammation Testing Predict Heart Disease Risk?
Yes — and this is one of the most valuable applications. hs-CRP testing has become a standard tool for cardiovascular risk stratification. The American Heart Association recognizes three risk categories: below 1 mg/L (low risk), 1–3 mg/L (moderate risk), and above 3 mg/L (high risk). A 2023 analysis in the European Heart Journal confirmed that elevated hs-CRP predicts heart attack and stroke risk independent of traditional factors like cholesterol and blood pressure. Importantly, this test is most useful for people at intermediate risk — it helps reclassify borderline cases into clearer risk categories. AHA/ACC CRP Guidelines [3] [9]
How Does Inflammation Testing Help Diagnose Autoimmune Conditions?
ESR and CRP together form the backbone of autoimmune disease monitoring. In conditions like rheumatoid arthritis, lupus, and polymyalgia rheumatica, inflammation markers help confirm diagnosis, assess disease activity, and guide medication adjustments. ESR tends to be particularly useful here because it reflects the chronic, sustained inflammation typical of autoimmune disorders. Serial testing — checking levels every 1–3 months during active disease and every 6–12 months during remission — helps clinicians catch flares early. [5]
Can Inflammation Markers Detect Hidden Infections?
Absolutely. CRP is especially valuable in emergency and hospital settings for distinguishing bacterial infections from viral ones. CRP levels above 50 mg/L are associated with acute bacterial infection approximately 90% of the time. This helps clinicians make faster decisions about antibiotic treatment. Post-surgically, CRP monitoring can detect complications like wound infections before obvious symptoms appear. [7]
What Can Inflammation Testing Tell You About Treatment Effectiveness?
Because CRP has a short half-life (about 19 hours), it responds quickly to successful treatment. If antibiotics are working, CRP drops within days. If an anti-inflammatory diet is reducing chronic inflammation, hs-CRP levels improve over weeks. This makes inflammation markers excellent tools for tracking whether your interventions — whether medications, lifestyle changes, or supplements — are actually making a difference.
Are There Any Risks or Limitations of Inflammation Testing?
Inflammation marker testing is safe from a medical standpoint — it involves a standard blood draw with minimal risks. However, there are significant interpretive limitations that can lead to misunderstanding, unnecessary anxiety, or missed diagnoses if you don't understand what the numbers can and can't tell you.

The biggest limitation is non-specificity. Elevated CRP tells you inflammation is present somewhere in the body. It does not tell you where the inflammation is, what's causing it, or how serious the underlying condition is. A CRP of 15 mg/L could mean a mild viral infection, a flaring autoimmune condition, or something more serious. Further diagnostic workup is always required.
What Are the Most Common False Positives?
Several non-disease factors can elevate inflammation markers and create misleading results:
- Obesity — Adipose tissue produces inflammatory cytokines. BMI above 30 commonly raises hs-CRP above 3 mg/L even without active disease
- Smoking — Chronic irritation raises CRP by 30–50% on average
- Intense exercise — A hard workout can temporarily spike CRP for 24–48 hours
- Stress — Chronic psychological stress elevates cortisol and inflammatory markers
- Recent illness — A cold or flu can keep CRP elevated for 1–2 weeks after symptoms resolve
- Medications — Hormone replacement therapy and oral contraceptives can raise CRP
- Age — ESR naturally increases with age, particularly after 50
Can You Have Inflammation With Normal Markers?
Yes — and this is an underappreciated limitation. Localized inflammation (like early-stage arthritis in a single joint) may not produce enough systemic signal to elevate blood markers. Immunosuppressive medications like corticosteroids and biologics can also suppress marker production, masking ongoing inflammation. A normal CRP does not definitively rule out inflammatory disease.

Should Everyone Get Inflammation Testing?
No. Routine screening in asymptomatic, low-risk individuals is not recommended because the high rate of false positives creates more confusion than clarity. Testing is most valuable when there's a clinical reason — suspected infection, autoimmune symptoms, cardiovascular risk assessment in intermediate-risk patients, or monitoring a known inflammatory condition.
How Do You Interpret Your Inflammation Test Results?
Interpreting inflammation markers requires understanding reference ranges, recognizing patterns across multiple markers, and — most importantly — considering your clinical context. Numbers without context are just numbers. Here's a practical framework for making sense of your results.
CRP and hs-CRP Reference Ranges
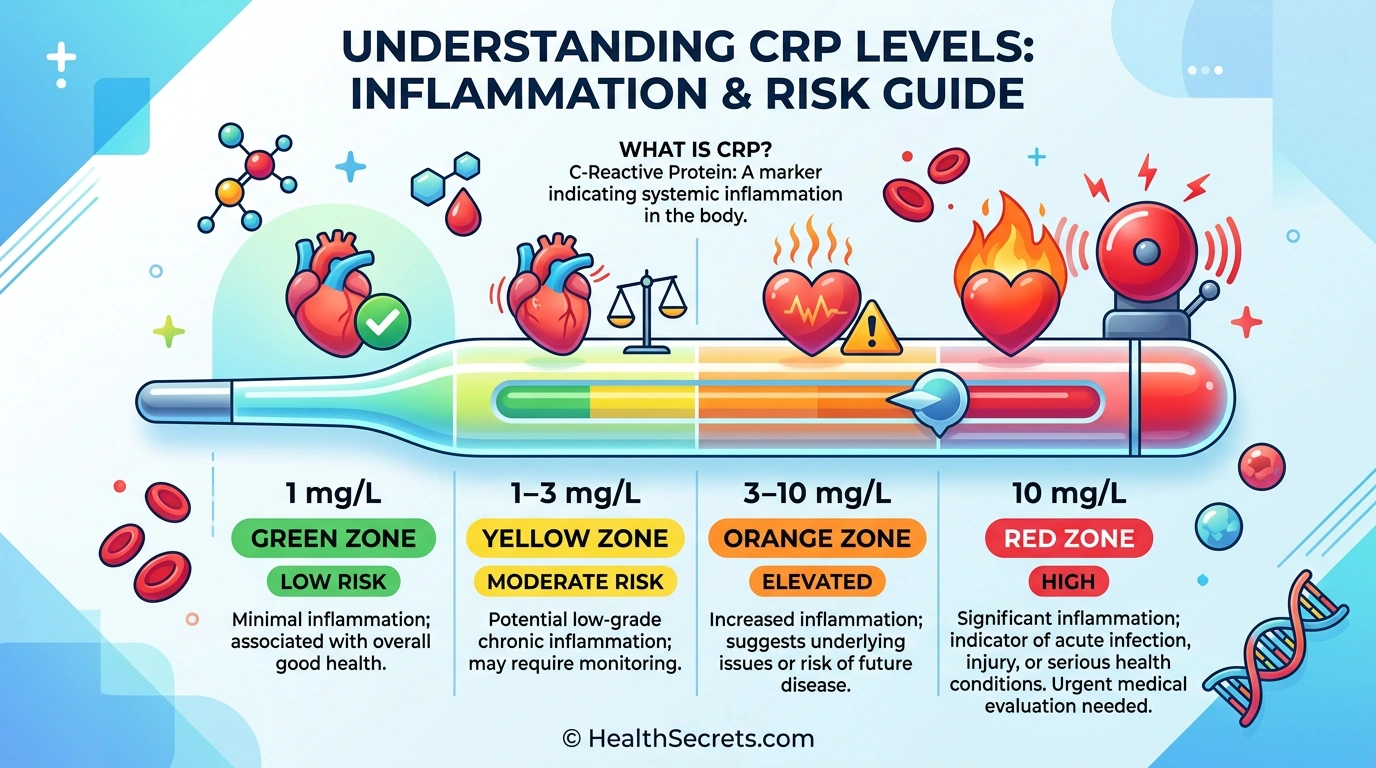
| Level | CRP (mg/L) | What It Suggests |
|---|---|---|
| Optimal | Below 1 | Low inflammation, low CVD risk |
| Mild elevation | 1–3 | Moderate CVD risk, possible low-grade inflammation |
| Elevated | 3–10 | Active inflammation, high CVD risk |
| Significantly elevated | 10–50 | Active infection or inflammatory condition |
| Severely elevated | Above 50 | Acute bacterial infection (~90% of cases) |
- Men under 50: Below 15 mm/hr
- Men over 50: Below 20 mm/hr
- Women under 50: Below 20 mm/hr
- Women over 50: Below 30 mm/hr
ESR increases naturally with age. Mild elevations in older adults may not be clinically significant.
Ferritin Reference Ranges
- Men: 30–200 ng/mL (optimal: 50–150 ng/mL)
- Women (premenopausal): 15–150 ng/mL (optimal: 30–100 ng/mL)
- Women (postmenopausal): 30–200 ng/mL
Remember: ferritin above 200 ng/mL in the presence of elevated CRP likely reflects inflammation, not iron overload. Ferritin below 30 ng/mL almost always indicates true iron deficiency, regardless of inflammation status.
Fibrinogen Reference Ranges
- Normal: 200–400 mg/dL
- Elevated: Above 400 mg/dL (increased CVD and clotting risk)
Key Interpretation Principles
- Look at patterns, not single numbers. A mildly elevated CRP with normal ESR suggests a different situation than both being significantly elevated.
- Repeat borderline results. A single mildly elevated hs-CRP should be confirmed with a repeat test 2 weeks later (after ruling out acute illness).
- Track trends over time. Serial measurements showing a downward trend are more meaningful than any single result.
- Consider the clinical picture. Always interpret results alongside symptoms, medical history, and physical exam findings.
- Rule out confounders. Before assuming disease, consider obesity, smoking, recent exercise, stress, or recent illness.
What Diet and Lifestyle Changes Help Reduce Elevated Inflammation Markers?
If your inflammation markers come back elevated — and your doctor has ruled out acute infection or a condition requiring medical treatment — the next step is addressing the modifiable factors that drive chronic inflammation. The evidence here is genuinely encouraging. Lifestyle changes can reduce CRP and other markers by 20–40% within 4–12 weeks.
What Should You Eat to Lower Inflammation?
The Mediterranean diet has the strongest evidence base for reducing inflammation markers. A pattern rich in vegetables, fruits, whole grains, fatty fish, nuts, seeds, and olive oil has been shown to reduce CRP by 20–30% in multiple clinical trials. Harvard Health: Foods That Fight Inflammation
Foods to emphasize:
- Fatty fish (salmon, sardines, mackerel) — omega-3 fatty acids directly reduce IL-6 and TNF-alpha
- Leafy greens (spinach, kale) — rich in antioxidants that neutralize oxidative stress
- Berries (blueberries, strawberries) — polyphenols with potent anti-inflammatory effects
- Extra virgin olive oil — oleocanthal has NSAID-like anti-inflammatory properties
- Nuts (walnuts, almonds) — healthy fats and vitamin E reduce inflammatory markers
- Turmeric and ginger — ginger for inflammation has clinical evidence for reducing CRP
Foods to minimize:
- Ultra-processed foods, refined carbohydrates, and added sugars
- Red and processed meats
- Trans fats and deep-fried foods
- Sugar-sweetened beverages
How Much Does Exercise Lower Inflammation?
Regular moderate exercise reduces CRP by approximately 20–30%. The key word is moderate — 150 minutes per week of activities like brisk walking, swimming, or cycling. Interestingly, a single intense workout can temporarily raise CRP, but consistent training over weeks produces a net anti-inflammatory effect. Johns Hopkins: Anti-Inflammatory Diet
Does Weight Loss Help?
Significantly. Losing just 5–10% of body weight can reduce CRP by 30–40%. Adipose tissue — especially visceral fat around your organs — actively produces inflammatory cytokines. Reducing that fat directly reduces the inflammatory signal. This is one of the most powerful single interventions for lowering chronic inflammation markers.
What About Supplements?
Several supplements have clinical evidence for reducing inflammation markers:
- Omega-3 fish oil (2–4g EPA+DHA daily) — reduces CRP, IL-6, and TNF-alpha by 20–30% in studies
- Curcumin (1,000–1,500mg daily with piperine) — reduces CRP and ESR, particularly in arthritis patients
- Vitamin D (1,000–2,000 IU daily if deficient) — deficiency is associated with elevated CRP
- Probiotics — emerging evidence for reducing systemic inflammation through gut health optimization
What Other Lifestyle Factors Matter?
- Sleep: 7–9 hours nightly. Chronic sleep deprivation (under 6 hours) significantly raises CRP and IL-6
- Stress management: Chronic stress elevates cortisol, which drives inflammation. Meditation, yoga, and deep breathing reduce markers measurably
- Smoking cessation: Quitting smoking reduces CRP by 30–50% within weeks
- Alcohol: Moderate or no consumption. Heavy drinking raises inflammation markers substantially
Action Plan
What Should You Do First If Your Inflammation Markers Are Elevated?
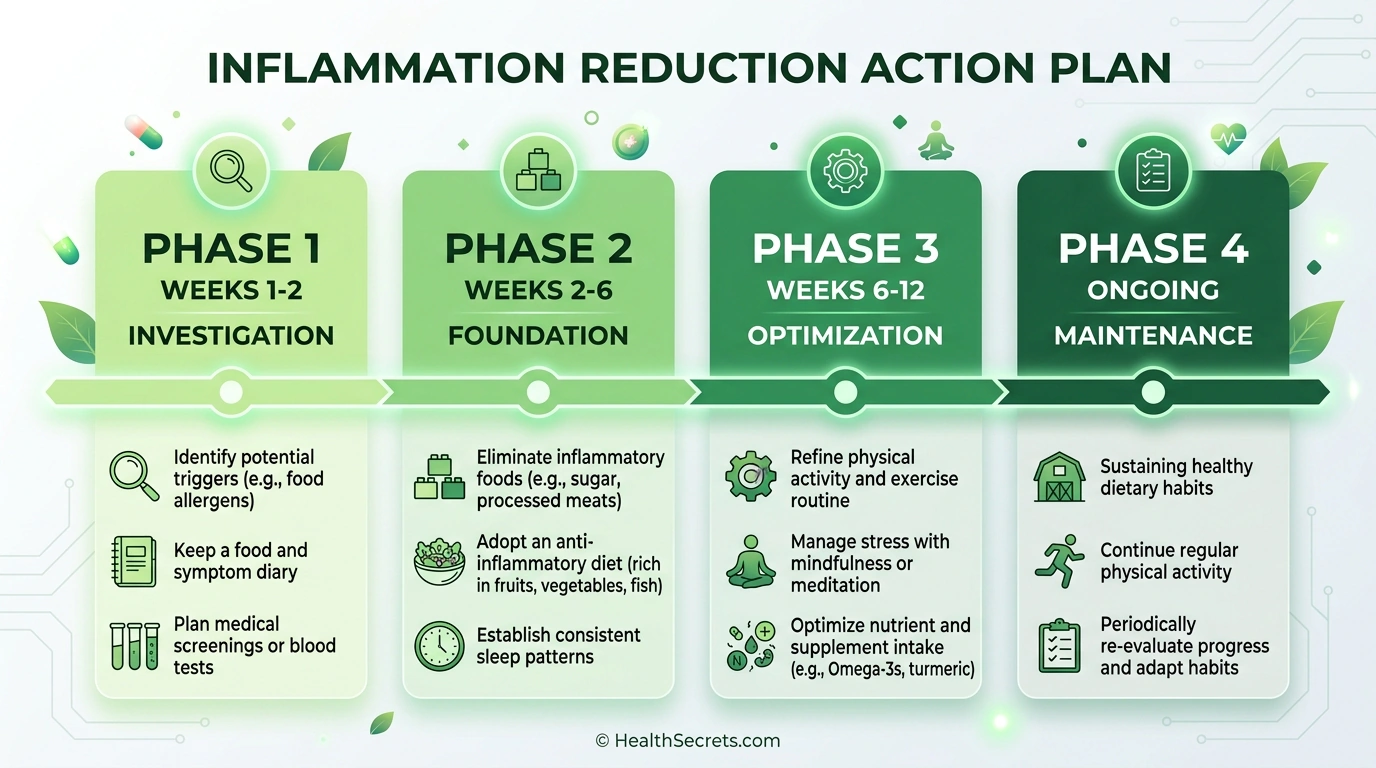
Follow the sequence below, work through each phase in order, and use the checklist as your practical implementation guide.
If you've received elevated inflammation test results, the most important first step is working with your healthcare provider to determine the cause — not just treating the number. Once acute conditions are ruled out, a phased lifestyle approach can bring chronic inflammation under control within 4–12 weeks.
Phase 1 — Immediate (Week 1–2):
- Review results with your healthcare provider to rule out infection, autoimmune disease, or other acute causes
- Identify and address obvious confounders — recent illness, medication effects, extreme stress
- Begin an anti-inflammatory dietary pattern (Mediterranean-style eating)
- If smoking, begin a cessation plan
Phase 2 — Foundation Building (Weeks 2–6):
- Establish consistent moderate exercise: 150 minutes/week (walking, swimming, cycling)
- Prioritize sleep: 7–9 hours nightly, consistent schedule
- Begin targeted supplementation if appropriate: omega-3 (2–4g EPA+DHA), vitamin D if deficient
- If overweight, begin gradual weight loss targeting 5–10% of body weight
- Implement daily stress management: 10–15 minutes meditation, deep breathing, or yoga
Phase 3 — Optimization and Monitoring (Weeks 6–12):
- Retest inflammation markers at 8–12 weeks to assess progress
- Adjust supplements and dietary strategies based on results
- Continue exercise progression
- If markers remain elevated despite lifestyle changes, discuss further medical evaluation with your provider
Phase 4 — Long-Term Maintenance:
- Retest every 3–6 months for ongoing monitoring
- Maintain anti-inflammatory lifestyle as a permanent foundation
- Track trends over time — the trajectory matters more than any single number